13 July 07 - Respiration and circulation during and after birth, ongoing...
Thurlow JA, Kinsella SM. Intrauterine resuscitation: active management of fetal
distress. Int J Obstet Anesth. 2002 Apr;11(2):105-16.
Ibrahim HM, Krouskop RW, Lewis DF, Dhanireddy R. Placental transfusion:
umbilical cord clamping and preterm infants. J Perinatol. 2000 Sep;20(6):351-4.
GAISFORD W. OBSTETRICS IN GENERAL PRACTICE. CARE OF THE
NEWBORN INFANT. Br Med J. 1964 Jul 4;2(5400):35-6.
Thurlow JA, Kinsella SM. Intrauterine resuscitation: active management of fetal
distress. Int J Obstet Anesth. 2002 Apr;11(2):105-16.
- Abstract: Acute fetal distress in labour is a condition of progressive
fetal asphyxia with hypoxia and acidosis. It is usually diagnosed by
finding characteristic features in the fetal heart rate pattern, wherever
possible supported by fetal scalp pH measurement. Intrauterine
resuscitation consists of applying specific measures with the aim of
increasing oxygen delivery to the placenta and umbilical blood flow, in
order to reverse hypoxia and acidosis. These measures include initial
left lateral recumbent positioning followed by right lateral or knee-elbow
if necessary, rapid intravenous infusion of a litre of non-glucose
crystalloid, maternal oxygen administration at the highest practical
inspired percentage, inhibition of uterine contractions usually with
subcutaneous or intravenous terbutaline 250 microg, and intra-
amniotic infusion of warmed crystalloid solution. Specific manoeuvres
for umbilical cord prolapse are also described. Intrauterine
resuscitation may be used as part of the obstetric management of
labour, while preparing for caesarean delivery for fetal distress, or at
the time of establishment of regional analgesia during labour in the
compromised fetus. The principles may also be applied during inter-
hospital transfers of sick or labouring parturients.
Ibrahim HM, Krouskop RW, Lewis DF, Dhanireddy R. Placental transfusion:
umbilical cord clamping and preterm infants. J Perinatol. 2000 Sep;20(6):351-4.
- OBJECTIVE: To investigate the clinical effects of early versus late cord
clamping in preterm infants. STUDY DESIGN: A total of 32 premature
infants were prospectively randomized. The following parameters were
measured: Initial spun hematocrit (Hct), hemoglobin (Hgb), red blood
cell (RBC) counts, frequency of blood transfusions, peak serum
bilirubin, mean blood pressure (MBP), oxygen index, intraventricular
hemorrhage, and significant patent ductus arteriosus (PDA).
RESULTS: Over the 4-week study period, the delayed cord clamping
(DCC) group exhibited a decrease in the frequency of blood
transfusion (p < 0.001) and also a decrease in albumin transfusions
over the first 24 hours (p < 0.03). MBP in the first 4 hours was higher in
the DCC group (p < 0.01), and there were statistically significant
increases in Hct (21%), Hgb (23%), and RBC count (21%) compared
with the early cord clamping group. The risks of patent ductus
arteriosus, hyperbilirubinemia, or intraventricular hemorrhage were
similar in both groups. Late clamping of the umbilical cord had little or
no effect on the oxygen index. CONCLUSION: DCC significantly
reduced the requirement for blood and albumin transfusion. It also
increased the initial Hct, RBC count, Hgb levels, and MBP.
GAISFORD W. OBSTETRICS IN GENERAL PRACTICE. CARE OF THE
NEWBORN INFANT. Br Med J. 1964 Jul 4;2(5400):35-6.
14 July 07 - Is autism a variant of kernicterus? Ongoing...
Shapiro SM. Definition of the clinical spectrum of kernicterus and bilirubin-
induced neurologic dysfunction (BIND). J Perinatol. 2005 Jan;25(1):54-9.
Langen M, Durston S, Staal WG, Palmen SJ, van Engeland H. Caudate Nucleus
Is Enlarged in High-Functioning Medication-Naive Subjects with Autism. Biol
Psychiatry. 2007 Jan 12 -- Biological Psychiatry, Volume 62, Issue 3, 1 August
2007, Pages 262-266.
Shapiro SM. Definition of the clinical spectrum of kernicterus and bilirubin-
induced neurologic dysfunction (BIND). J Perinatol. 2005 Jan;25(1):54-9.
- There have also been suggestions of a relationship of moderate
levels of hyperbilirubinemia to the subsequent development of
other disorders such as attention deficit hyperactivity disorder
(ADHD), Parkinson disease, and even autism, but so far, there is
no evidence to support these contentions. [p 57]
- Auditory-predominate kernicterus may manifest as moderate or
severe AN, with or without a hearing loss, with minimal or mild
motor symptoms and perhaps a normal or slightly abnormal
globus pallidus or a subthalamic nucleus as seen in MRI. [p57]
Langen M, Durston S, Staal WG, Palmen SJ, van Engeland H. Caudate Nucleus
Is Enlarged in High-Functioning Medication-Naive Subjects with Autism. Biol
Psychiatry. 2007 Jan 12 -- Biological Psychiatry, Volume 62, Issue 3, 1 August
2007, Pages 262-266.
- IN THIS ISSUE-AUGUST 1ST
Abnormal Patterns of Brain Development in Autism
Langen et al. (pages 262–266) investigated the involvement
of the basal ganglia in autism. They examined magnetic
resonance imaging (MRI) brain scans from two independent
samples of children and adolescents with autism and matched controls
and found enlarged caudate nucleus volumes in the autism group in
both samples. As both samples were medication-naive, this implicates
the basal ganglia in the expression of this disorder.
17 July 07 - Myers patterns of perinatal brain damage
Myers RE. Two patterns of perinatal brain damage and their conditions of
occurrence. Am J Obstet Gynecol. 1972 Jan 15;112(2):246-76.
Myers RE. Four patterns of perinatal brain damage and their conditions of
occurrence in primates. Adv Neurol. 1975;10:223-34.
Myers RE. Two patterns of perinatal brain damage and their conditions of
occurrence. Am J Obstet Gynecol. 1972 Jan 15;112(2):246-76.
- Excerpts:
- "Term monkey fetuses are exposed to rigorously timed episodes of
total asphyxia by slipping a thin, saline-filled, rubber sac over the fetal
head at surgical delivery and clamping the umbilical cord. The
envelopment of the fetal head prevents the onset of air breathing while
the clamping of the umbilical cord abruptly halts fetal placental
circulation." [p247]
- "The first evidence for damage to the brain following resuscitation and
extended survival occurs in unanesthetized term fetuses subjected to
10 min. of total asphyxia. Term fetuses asphyxiated for longer than 25
min. die in the early hours in the intensive care u nit of progressive and
intractable heart failure due to injury of the myocardium" [p251]
"The brain center earliest damaged are the inferior colliculi as
illustrated in Fig. 3. Thereafter, in a monotonously repetitive rank
order, follow other brainstem structures including the superior olives,
the sensory nuclei of the trigeminal nerve, the gracile and cuneate
nuclei, the medial and spinal vestibular nuclei, and the posterior and
lateral ventral thalamic nuclei. These structures are injured by
asphyxial episodes lasting for only 10 to 13 min." [p251]
"The ultrastructural changes include mitochondrial shrinkage and loss
of the structural integrity of all constituent membranes. The cell-limiting
membrane appears most sensitive in this regard while the nuclear
membrane is most resistant.
... Zones of destructive change after a time lag, stimulate an infiltration
of mononuclear cells from the bloodstream.
... The rank order of involvement of the various brainstem structures
following total asphyxia remains constant from animal to animal" [p253]
"The ranking of brain structures in their order of susceptibility to injury
following total asphyxia duplicates, in general, their ranking with regard
to their volume flow of blood per unit time as determined by 14C-
labeled antipyrine diffusion studies. The inferior colliculus, the
structure most outstandingly vulnerable to total asphyxia, is also the
structure most highly perfused with blood (fig. 7 - see below).
... The brainstem injury pattern produced in the monkey fetus by total
asphyxia bears no relation to the brain pathology typifying human
perinatal damage. In actuality, this distinctive brainstem injury pattern
appears only rarely in the human brain. When seen, it appears almost
exclusively in infants or young children following cardiac arrest." [p254]
"The fetus, still in uter, may be subjected to an entirely different type of
asphyxial assault characterized by a partial rather than a total
interference with its respiratory gas exchange." [p256]
"In utero, partial asphyxia of the fetus may be brought about in a variey
of ways. Infusion of excessive oxytocin into the maternal bloodstream
was the method first used experimentally in our laboratory.
... Subsequently, fluorothane hypotension, mechanical constriction of
the maternal abdominal aorta, and experimental partial placental
ablation have also proved effective in producing asphyxia.
... The greatest experience has been achieved with maternal aortic
constriction." [p257]
IN PROGRESS...
Myers RE. Four patterns of perinatal brain damage and their conditions of
occurrence in primates. Adv Neurol. 1975;10:223-34.
- Abstract: The findings described in the present study are summarized
in Table 1. It may be noted that anoxia or total asphyxia, whether in the
newborn animal or in the (see article) adult, leads to patterns of injury
in the brainstem. Hemispheral structures outside the thalamus seem to
be entirely spared in those animals which survive. In contrast to this,
situations leading to hypoxia associated with severe acidosis, usually of
a mixed respiratory and metabolic type, cause brain edema; and when
the edema is limited in its distribution, the damage is restricted to
specific cortical loci. When the cerebral edema becomes more
generalized owing to spread of the process, more and more extensive
regions of the hemispheres are damaged until the entire cerebrum may
become necrotic. On the other hand, clinical circumstances which lead
to hypoxia but without acidosis of any great magnitude--usually due to
the indolence of the process or to an associated hyperventilation of the
mother--produce lesions which may be restricted to the white matter.
These processes may be characterized by perivenular white matter
hemorrhage and/or focal areas of periventricular leucomalacia. Finally,
those clinical circumstances which lead to combined episodes of
hypoxia plus anoxia with acidosis favor a predominance of lesions that
affect the basal ganglia.
18 July 07 - Milieu Research, and visit from Cardinal Sean O'Malley
Assigned to work in our Intensive Treatment Unit (ITU) today, a gray rainy day, with
several patients in acute distress. I went out to check up on a patient who has
been refusing to eat or drink, and reluctant to talk with anyone. To my surprise,
there was Cardinal Sean O'Malley of the Catholic Archdiocese of Boston,
bestowing a blessing on this patient. Our hospital superintendent, Karin Bergeron,
introduced me to Cardinal O'Malley, who then spoke briefly with me, and told me
he spent two years as a prison chaplain. This was a very moving experience --
and the patient appeared much less despondent later this afternoon, and
agreeable to finally trying a medication he has steadfastly been refusing.
Assigned to work in our Intensive Treatment Unit (ITU) today, a gray rainy day, with
several patients in acute distress. I went out to check up on a patient who has
been refusing to eat or drink, and reluctant to talk with anyone. To my surprise,
there was Cardinal Sean O'Malley of the Catholic Archdiocese of Boston,
bestowing a blessing on this patient. Our hospital superintendent, Karin Bergeron,
introduced me to Cardinal O'Malley, who then spoke briefly with me, and told me
he spent two years as a prison chaplain. This was a very moving experience --
and the patient appeared much less despondent later this afternoon, and
agreeable to finally trying a medication he has steadfastly been refusing.
18 July 07 - Myers' Two Patterns excerpts, continued
Myers RE. Two patterns of perinatal brain damage and their conditions of
occurrence. Am J Obstet Gynecol. 1972 Jan 15;112(2):246-76.
Figures 19 and 7 below, from Myers (1972) paper, show how blood flow in the
brain is affected by what he termed "partial asphyxia," or oxygen insufficiency
caused by impaired maternal circulation to the placenta (figure 19). With
diminished oxygen, circulation to the inferior colliculi and other brainstem nuclei
of high metabolic rate is increased (a protective mechanism), while blood flow to
the metabolically less active cerebral cortex is severely diminished.
Compare figure 19 B with figure 7, showing normal blood flow pattern, which is
highest in the brainstem, especially the inferior colliculi.
Myers RE. Two patterns of perinatal brain damage and their conditions of
occurrence. Am J Obstet Gynecol. 1972 Jan 15;112(2):246-76.
- "Alterations in blood flow in the brains of term monkey fetuses
subjected to in utero partial asphyxia have been objectively
demonstrated with the use of 14C-labeled antipyrine (Reivich M et al. in
Meyer JS, ed, Research on the cerebral circulation, Fourth Salzburg
Conference on Cerebral Flow, 1970, LOC call # RC388.5 .I5 1968).
These studies show that the brunt of blood flow alterations is felt by the
hemispheres." [p265]
"When an episode of partial aspphyxia endures for from 1/2 hr. to
several hours (depending on its severity), injury to the fetal brain may
result. The observed patterns of injury are variable and form a
spectrum extending from, at one extreme, a total hemispheral necrosis
(fig 21), usually associated with a failure to survive beynond the first
hours of birth, to circumscribed damage to the middle third of the
paracentral cortical region (fig 22).
... Animals with restricted injury may also die early or may survive into
adult life as palsied individuals.
... basal ganglia damage may occur both with or without concomitant
injury to the cerebral cortex.
... When episodes of total asphyxia are superimposed upon episodes
of partial asphyxia, the characteristic brainstem injury pattern may also
be manifest." [p267]
... "The close similarities between the brain pathology of in utero partial
asphyxia in the monkey and the pathology of cerebral palsy in the
human being suggest that in utero partial asphyxia may play a major
role in the pathogenesis of cerebral palsy in the human being.
... No treatment can recover the usefulness of cerebral tissue which
has become necrotic following the development of brain swelling and
the exclusion of cerebral circulation. Thus the combination of
depressed consciousness, decerebrate posturing, seizures, bulging
fontanels, and retinal hemorrhages in the newly born infant associated
with a history of asphyxia during birth bespeaks a grave prognosis."
[p269]
"All delivery rooms and infant intensive care units should be provided
with ventilators designed for human infant use
... However, the lungs of newborn infants, particularly of premature
ones, may be overinflated to the point of mechanical injury...." [p 272]
"Following asphyxia, cardiovascular performance may be so depressed
that it provides the infant with little or no circulation despite ECG
evidence of heart action. Under such circumstances, the institution of
artificial pulmonary ventilation alone is without result. The second step
of crucial importance, then, is the provision of a sufficient blood flow to
return the oxygenated by stagnant blood to the heart." [p273]
Figures 19 and 7 below, from Myers (1972) paper, show how blood flow in the
brain is affected by what he termed "partial asphyxia," or oxygen insufficiency
caused by impaired maternal circulation to the placenta (figure 19). With
diminished oxygen, circulation to the inferior colliculi and other brainstem nuclei
of high metabolic rate is increased (a protective mechanism), while blood flow to
the metabolically less active cerebral cortex is severely diminished.
Compare figure 19 B with figure 7, showing normal blood flow pattern, which is
highest in the brainstem, especially the inferior colliculi.
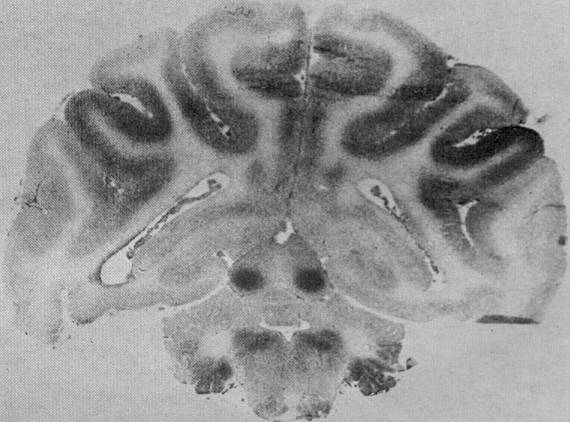
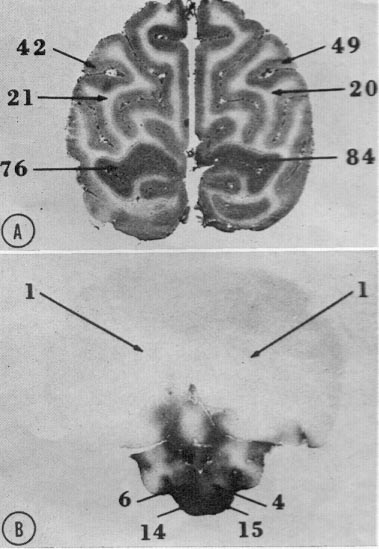
Fig 19. Autoradiographs
demonstrating alterations
in fetal cerebral blood flow
produced by in utero fetal
partial asphyxia. The fetus
exposed to less severe
asphyxia (A) exhibited
decreases in blood flow
throughout major extents of
the cortical gray matter and
the centrum semiovale.
Only the striated cortex
region manifested
minimally in the way of
blood flow alteration. In
some areas, blood flow
reductions as large as 50
percent are observed in
this brain. With the
development of severe
hemispheral swelling as
indicated by the
compressions of the
superior cerebellar
surfaces, a total loss in
hemispheral perfusion
results (B). while the
brainstem is little affected,
the cerebellum may exhibit
symmetrical zones of
diminished perfusion.
demonstrating alterations
in fetal cerebral blood flow
produced by in utero fetal
partial asphyxia. The fetus
exposed to less severe
asphyxia (A) exhibited
decreases in blood flow
throughout major extents of
the cortical gray matter and
the centrum semiovale.
Only the striated cortex
region manifested
minimally in the way of
blood flow alteration. In
some areas, blood flow
reductions as large as 50
percent are observed in
this brain. With the
development of severe
hemispheral swelling as
indicated by the
compressions of the
superior cerebellar
surfaces, a total loss in
hemispheral perfusion
results (B). while the
brainstem is little affected,
the cerebellum may exhibit
symmetrical zones of
diminished perfusion.
Fig. 7. Autoradiograph of coronal brain section of normal newborn monkey. Just prior to being killed,
this animal sustained an intravenous infusion of 14C-labeled antipyrine. Staining density relates to
volume flow of blood per unit of tissue per unit of time. The central nuclei of the inferior colliculi stand out
due to their high-volume blood flow. (Courtesy C. Kennedy and L. Sokoloff, Laboratory of Cerebral
Metabolism, National Institute of Mental Health.)
this animal sustained an intravenous infusion of 14C-labeled antipyrine. Staining density relates to
volume flow of blood per unit of tissue per unit of time. The central nuclei of the inferior colliculi stand out
due to their high-volume blood flow. (Courtesy C. Kennedy and L. Sokoloff, Laboratory of Cerebral
Metabolism, National Institute of Mental Health.)
21 July 2007 - Alex F. Robertson on errors in neonatology, III
Robertson AF.Reflections on errors in neonatology III. The "experienced" years,
1970 to 2000. J Perinatol. 2003 Apr-May;23(3):240-9.
Excerpts:
ERYTHROMYCIN
PROPYLENE GLYCOL
BENZYL ALCOHOL
INTRAVENOUS (I.V.) VITAMIN E
STEROIDS
Robertson AF.Reflections on errors in neonatology III. The "experienced" years,
1970 to 2000. J Perinatol. 2003 Apr-May;23(3):240-9.
Excerpts:
- NEO-MUL-SOY FORMULA
- "One of the swiftest responses to an error began on July 26, 1979
when three cases of failure to thrive and metabolic alkalosis were
reported to the Center for Disease Control (CDC). All three infants
were being fed a soy-based formula, Neo-Mul-Soy. On July 30, CDC
investigators surveyed a sample of pediatric nephrologists in the US
and found an additional 15 cases and another 16 cases from other
sources. All the infants had received either Neo-Mul-Soy or Cho-
Free, formulas produced by the same company. By August 2, the
company had analyzed the suspect formulas, met with the FDA,
halted manufacture, ordered a recall, and notified health-care
professionals throughout the country about the problem.7
Fortunately, the children recovered quickly when supplemented
with another formula or chloride.
The most complete discussion of the epidemic is contained in
an article by Dr. Shane Roy, the originator of the initial report
to the CDC.8 The metabolic alkalosis was caused by the renal
effects of chloride deficiency." [pp240-241]
"The factors leading to the deficiency of chloride in the formula
are very interesting. In the 1950s and 1960s, the concern surfaced
that hypertension might result from increased sodium intake in
infancy.9 Although this correlation was never verified, in 1971 the
American Academy of Pediatrics (AAP) recommended that the ‘‘salt
content’’ of infant foods be reduced." [p241]
ERYTHROMYCIN
- "In February 1999, in Knoxville, TN, there was an outbreak of
pertussis involving six newborn infants. Since the most likely
source of infection was a hospital worker, the local health
department suggested prophylaxis of about 200 infants who may
have been exposed to that worker. The prophylaxis was the
antibiotic erythromycin as recommended by the American Academy
of Pediatrics.25 Approximately 6 weeks later, local pediatric
surgeons had a cluster of seven cases of pyloric stenosis, all of
whom had been born in the hospital where the erythromycin was
given and all had received the drug.26 The results of a cohort study
showed that none of the infants who had not received erythromycin
in that time period developed pyloric stenosis." [p241]
PROPYLENE GLYCOL
- "In 1983, Glasgow et al.36 reported four infants with serum
hyperosmolality (4300 mosm/l) related to elevated levels of
propylene glycol in the blood. The source was a parenteral
multivitamin preparation (MVI-12) containing propylene glycol. As
mentioned in the article, the authors had changed multivitamin
preparations in their NICU to one containing biotin and had
increased the volume of vitamin solution given to provide adequate
amounts of the other vitamins.36 This change led to a 10-fold
increase in the propylene glycol dose. The vitamin preparation used
was not recommended for patients under 11 years of age." [p243]
BENZYL ALCOHOL
- "In 1981, at the SSPR meeting Gershanik et al.38 reported five
preterm infants with severe metabolic acidosis, hepatic and
renal failure, and signs of neurological deterioration. A striking
clinical aspect was the onset of gasping respirations and the
authors named the illness the ‘‘gasping’’ syndrome. Unmetabolized
benzyl alcohol was found in the urine. An additional 10 babies
with the ‘‘gasping’’ syndrome died in Oregon that year and were
reported by Brown et al.39 The infants were all of very low birth
weight, in the first days of life and had central venous catheters
(umbilical artery and/or vein) that were flushed frequently using
bacteriostatic normal saline containing 0.9% benzyl alcohol. These
cases were reported to the FDA, which recommended the exclusion
of benzyl alcohol from flush solutions and diluents used in
newborns." [p243]
"On May 28, 1982, the Food and Drug Administration (FDA) sent
letters recommending that flush solutions used in newborns should
not contain benzyl alcohol or any other preservative." [p244]
INTRAVENOUS (I.V.) VITAMIN E
- "In 1949, before the implication of oxygen as a cause of retrolental
fibroplasia (RLF), Owens and Owens56 postulated that RLF
was related to vitamin E deficiency.
...Although further trials during the 1970s on the efficacy of
vitamin E in ameliorating RLF were conflicting, many nurseries
administered the vitamin orally to their premature infants.
... In December 1983,
E-Ferol Injection for intravenous administration was introduced
... Within months of E-Ferol’s introduction to neonatal care,
neonatologists began to note clusters of premature babies who
developed hepatomegaly, thrombocytopenia, cholestatic jaundice,
ascites, and azotemia.
... On
April 16, 1984, the FDA issued an Urgent Class I Drug Recall letter,
indicating that the drug was being voluntarily recalled by the
company." [pp244-245]
STEROIDS
- "There is controversy about the relation between steroid therapy
(used for the treatment or prevention of bronchopulmonary
dysplasia (BPD)) and cerebral palsy." [p245]
"BPD was first described by Northway et al.68 in 1967.
With improvements in infant ventilators, more small infants
survived and more infants had chronic lung disease. BPD was
(and still is) the greatest disappointment in neonatal care..." [p246]
" ... I was ready to accept any treatment and
remember exactly when I started using corticosteroids. The year
was 1985 and Dr. Spencer Brudno had just joined our faculty. In
January, he had co-authored with Avery, Fletcher, and Kaplan an
article describing the beneficial results of dexamethasone in infants
with BPD.69 The treatment caused improvement in pulmonary
compliance and rapid weaning from the respirator. This early
study, and the few preceding it, did not provide developmental
follow-up data." [p246]
"Yeh et al.74 in 1998 and O’Shea et al.75 in 1999 showed an increase
in neuromotor dysfunction and cerebral palsy in dexamethasone treated
infants. An excellent review of the many aspects of this
question is presented by Watterberg.
Evaluating this subject as a possible error is difficult at this
time and this discussion is not complete. Infants with BPD are at
risk for poor neurodevelopmental outcome regardless of the
treatment." [p246]
- "In all these episodes, excluding the vitamin E tragedy, the
motivation leading to harmful treatments was an honest desire to
improve the care of infants." [p246]
"Many of these events, regardless of the process error, have
resulted from the use of pharmacological agents (synthetic vitamin
K, sulfisoxazole, chloramphenicol, novobiocin, hexachlorophene,
erythromycin). New pharmacological agents have been and will
continue to be a danger in neonatology. Many adverse effects may
not be seen in small population studies performed for licensing." [p247]
"The greatest hazard since the ‘‘Hands Off’’ years has been
unexpected reactions to drugs." [p247]
"I hope that by studying these mistakes, we will avoid some
future problems or at least recognize the problems early in their
course." [p247]
23 July 2007 - Alex F. Robertson on errors in neonatology, II
Robertson AF.Reflections on errors in neonatology: II. The "Heroic" years, 1950 to
1970. J Perinatol. 2003 Mar;23(2):154-61.
In this paper, Robertson summarized innovations in neonatal care that had come
about since the 1920s. Most notable were (1) exchange transfusions for infants with
"Rh isoimmunization," and (2) use of antibiotics.
In this paper Robertson also discussed the Bloxsom air-lock incubator, epsom salt
enemas, the antibacterial soap Hexachlorophene, laundry detergents, and
disinfectant cleaning agents.
Excerpts:
Robertson AF.Reflections on errors in neonatology: II. The "Heroic" years, 1950 to
1970. J Perinatol. 2003 Mar;23(2):154-61.
In this paper, Robertson summarized innovations in neonatal care that had come
about since the 1920s. Most notable were (1) exchange transfusions for infants with
"Rh isoimmunization," and (2) use of antibiotics.
- (1) Rh isoimmuniaztion had formerly been known as erythroblastosis fetalis,
or jaundice and anemia caused by destruction of red blood cells of the
infant by maternal antibodies to the Rh factor.
By the 1960s, RhoGam (or anti-D) immune globulin had been developed,
which given to an Rh-negative mother after the birth of her first child,
prevents formation of anti-bodies to the Rh factor. The maternal-placental
barrier prevents any fetal blood from getting into the mother's circulation
throughout gestation. It appears unquestioned why this barrier is breached
during the process of birth, but clamping of the umbilical cord (also
unquestioned as possibly dangerous) suddenly shuts off blood flow from
the placenta to the newborn infant. Blood backing up in the placenta
causes bursting of capillaries, with leakage of fetal blood into the mother's
blood stream. Waiting for the placenta to be born, with the umbilical cord
intact, allows placental blood to be completely transferred to the infant.
Placental blood is respiratory blood, and would appear by nature's plan
intended to be transferred to the capillaries that supply the infant's alveoli.
Carbon dioxide previously exchanged for oxygen in the placenta is then
released into the alveoli for exhalation. The first breath then refills the
alveoli newly expanded by carbon dioxide. For more on reflexes involved in
breathing, see Marsh MJ et al. Pediatr Pulmonol. 1994 Sep;18(3):163.
What human hubris ever led to interference with this plan for all placental
mammals?
(2) Antibiotic medications had been enthusiastically adopted without any
question of how they might produce adverse reactions. However,
antibiotics disrupt metabolism in bacteria, and they likewise can disrupt
metabolism in mitochondria, which are thought to have been a primeval
symbiotic inclusion (or infection) in early multicelluar organisms, symbiotic
because they contain enzymes of aerobic metabolism. See for instance
Zhang L et al. FEBS Lett. 2005 Nov 21;579(28):6423.
In this paper Robertson also discussed the Bloxsom air-lock incubator, epsom salt
enemas, the antibacterial soap Hexachlorophene, laundry detergents, and
disinfectant cleaning agents.
Excerpts:
- "These years were
exciting. Silverman (1) refers to ‘‘therapeutic exuberance’’; Baker
describes a ‘‘great spirit of innovation, somewhat lacking in
discipline’’ and refers to the ‘‘heroic’’ era (2). All treatments were
new, untested, and we marched on without fear! As a result of our
uncritical enthusiasm for treatment, many errors occurred." [p154]
(1) Silverman WA. Retrolental Fibroplasia: a modern parable. New York:
Grune & Stratton, 1980.
ANTIBIOTIC ERRORS
"In 1879, Pasteur demonstrated bacteria in the
blood and lochia of puerperal sepsis victims. The organism was
Group A Streptococcus. The use of careful antiseptic practices was
the only recourse against infection until the introduction of
sulfonamides in the 1930s and then penicillin in the 1940s." [p155]
"In 1953, a newly available sulfonamide,
sulfisoxazole, was introduced and had the advantage of requiring
less frequent dosing to maintain adequate blood levels. No
problems were recognized with its use. When the use of
subcutaneous oxytetracyclene was suggested, a controlled study was
begun comparing this drug to the accepted regimen of penicillin
and sulfisoxazole. ‘Much to our amazement, the first trial gave a
definitive result. To our horror, the mortality rate was highest (and
strikingly so) in infants who received the established treatment!’
The cause of the increased mortality rate was kernicterus which, at
autopsy, was nine times increased." [p155]
"Sutherland published the first description of three cases of
cardiovascular collapse in newborn infants receiving large doses of
chloramphenicol. The infants were treated because of prolonged
rupture of the membranes and concern about infection. A few days
after the treatment began, the infants developed abdominal
distention, slate-colored or pallid cyanosis (the ‘gray baby’
syndrome), cold moist skin, and weak pulse; they died shortly
thereafter." [p156]
"... The tragic
practice of using chloramphenicol ended in about 1960 as these
reports became common knowledge in medical circles." [pp156-157]
"In 1959, there was a staphylococcal infection epidemic in a
term newborn nursery at the Cincinnati General Hospital. To abort
the outbreak, novobiocin was given to all infants admitted to the
nursery since the organism was resistant to penicillin and
erythromycin. An increase in the number of infants with
hyperbilirubinemia was quickly noted by Dr. Sutherland, who had
earlier been one of the first to recognize chloramphenicol toxicity...
... Fortunately, none of the infants in the Cincinnati epidemic
developed kernicterus during their hospitalization and only 12
babies required exchange transfusion. It was fortunate that this
effect was recognized before the drug was used widely in newborn
infants." [p157]
EQUIPMENT CLEANING
"In 1972, doctors at a New Jersey hospital performed five exchange
transfusions for hyperbilirubinemia in a period of 36 hours...
... Staff members
reported that, in preparation for one of their colleagues delivery,
they cleaned the bassinet reserved for that baby several times with
their routine disinfectant detergent (Vestal LpH, Vestal Laboratories,
St. Louis MO). That baby needed three exchange transfusions for
jaundice. This led to an investigation of the disinfectant which
contained several phenolic compounds. " [p160]
"These cases demonstrate the
unique susceptibility of newborn infants. As the investigators
mention,56 newborn infants absorb materials easily through their
epidermis. Also, their respiratory rate is higher than adults so
newborn infants may inhale larger amounts of environmental
contaminants." [p160]
24 July 2007 - Alex F. Robertson on errors in neonatology, I
Robertson AF. Reflections on errors in neonatology: I. The "Hands-Off" years, 1920
to 1950. J Perinatol. 2003 Jan;23(1):48-55.
Excerpts:
Comments:
(1) More on retinopathy of prematurity. Is ischemia the real cause? See, for
example, Jandeck C et al. Retinopathy of prematurity in infants of birth weight > 2000
g after haemorrhagic shock at birth. Br J Ophthalmol. 1996 Aug;80(8):728-31.
(2) Blood-brain barrier damage is more likely the real cause of kernicterus, from
multiple toxic factors, or ischemia. Bilirubin is not directly disruptive to the blood-
brain barrier, but stains the nuclei in which the blood-brain barrier has been
breached. More and more on this ongoing...
Robertson AF. Reflections on errors in neonatology: I. The "Hands-Off" years, 1920
to 1950. J Perinatol. 2003 Jan;23(1):48-55.
Excerpts:
- SUPPLEMENTAL OXYGEN
- "However, as the survival of smaller infants improved, the
incidence of RLF continued to be significant in very small premature
infants and was renamed retinopathy of prematurity (ROP) to
indicate its relation to gestational age. The search for ROP’s etiology
continues." [p 52]
- SMA FORMULA CHANGE
- "In December 1952, the FDA received a letter from a nurse in Arkansas
whose 3-month- old infant had developed convulsions. The
attending pediatrician apparently suspected that the condition was
related to the formula, SMA liquid. The formula was changed to an
evaporated milk formula and the child recovered. The mother heard
of eight similar cases and that led to her letter. Upon further
investigation, the FDA found that the manufacturer had heard of the
problem and knew of 12 cases.
... A detailed review of several additional
cases showed only one common factor: the infants had all been fed
liquid SMA formula and no solids.
... As SMA was the presumed culprit, the FDA began extensive
investigations for toxic materials.
Vitamin assays were performed and the level of
vitamin B6 was found to be quite low. Wyeth sent a general notice to
all physicians describing this problem with their formula. A national
survey revealed 300 cases of formula- induced vitamin B6
deficiency." [p53]
- SYNTHETIC VITAMIN K PROPHYLAXIS
- "The prophylactic use of vitamin K in newborns began in the early
1940s and was the second routine pharmacological treatment of
newborn infants; the first being the use of silver nitrate to prevent
ophthalmia neonatorum begun by Crede´ in 1881. In 1954, the
American Academy of Pediatrics recommended a dose of 5 mg of
synthetic vitamin K for all newborn infants."
"In 1955, Allison,42 in a short letter to The Lancet, mentioned his
experience of seeing cases of hemolytic anemia, hyperbilirubinemia,
and kernicterus in premature infants treated with large doses of
synkavit, a water - soluble vitamin K analogue. ...
... I can find no publication that gave a rationale for or advocated
the use of increased doses of vitamin K. Again, it is impossible to
quantitate the damage done but, considering the broad use of large
doses of synthetic vitamin K and the years of use (1945–1961), I
believe it was extensive." [p53]
Comments:
(1) More on retinopathy of prematurity. Is ischemia the real cause? See, for
example, Jandeck C et al. Retinopathy of prematurity in infants of birth weight > 2000
g after haemorrhagic shock at birth. Br J Ophthalmol. 1996 Aug;80(8):728-31.
(2) Blood-brain barrier damage is more likely the real cause of kernicterus, from
multiple toxic factors, or ischemia. Bilirubin is not directly disruptive to the blood-
brain barrier, but stains the nuclei in which the blood-brain barrier has been
breached. More and more on this ongoing...