29-30 May 07 - Research on continuing placental circulation after birth
In progress... Research on delayed versus the current standard of immediate
clamping of the umbilical cord is based on "randomized controlled trials," and how
ethical this may be should be questioned. Below are citations to research going
back over 130 years that should provide all the evidence needed that clamping the
umbilical cord should not be done, or at least not until the newborn infant is
breathing, especially in cases of difficult and traumatic births. These references
were taken from notes put together while working on posters for the Fetal and
Neonatal Society (FNPS) conference last September. The notes are at:
http://www.inferiorcolliculus.org/fnps01.html
Included below are references on influences such as umbilical cord blood banking,
which began in the 1930s, ideas about infant death following Cesarean delivery,
Jäykkä's research on lung expansion following filling of the capillaries around the
alveoli, cardiac murmurs indicating failure of full transition from fetal to neonatal
circulation, and reports of ischemic brainstem damage observed in human infants
resembling the damage found in monkeys and thoroughbred foals delivered with
human interventions (including clamping of the umbilical cord):
- Budin, P (1875) A quel moment doit-on pratiquer la ligature du cordon
ombilical? Progres Medical 3:750-751, 765-767, (1876) 4:2-3.
- Schucking, A (1877) Zur Physiologie der Nachgeburtsperiod.
Untersuchungen ueber den Placentarkreislauf nach der Geburt des Kindes.
Berliner Klinishe Wochenschrift 1877 #1 (1 Jan):5-7 and (8 Jan):18-21.
- Ziegler CE (1922) Additions to our obstetric armamentarium. Am J Obstet
Gynecol 3:46-53
- Haselhorst G (1928a) Zum plazentaren Kreislauf unter der Geburt. Zeitshrift
fur Gegurtshulfe und Gynakologie 95:32-42.
- Haselhorst G (1928b) Zum plazentaaren Kreislauf unter der Geburt. Zeitshr. f.
Geb. u Gynakol. 95:224-233.
- Haselhorst G (1929) Uber Art und Dauer der Blutstromung in den
Nabelschnurgefassen post partum. Z Geburtshilfe Gynakol 96:487-499
(Zeitschrift für Geburtshilfe und Gynäkologie)
- Allmeling A (1930) Die Gewichtszunahme von Neugeborenen infolge
postnataler Transfusion. Zentralblatt fur Gynakologie 54(14):850-860.
- Haselhorst G, Allmemling A (1930) Die Gewichtszunahme von Neugeborenen
infolge postnataler Transfusion. Zeitshrift fur Gegurtshulfe und Gynakologie
98:103-104.
- Goodall JR, Anderson FO, Altimas GT, MacPhail FL (1938) An inexhaustible
source of blood for transfusion and its preservation. Surgery, Gynecology
and Obstetrics 66:176-178.
- Frischkorn HB , Rucker MP (1939) The relationship of the time of ligation of
the cord to the red blood count of the infant. Am J Ostet Gynecol 38:592-594.
- Barton FE, Hearne TM (1939) The use of placental blood for transfusion.
JAMA 113:1475-1478.
- Grodberg BC, Cary EL (1939) A study of seventy-five transfusions with
placental blood. New England Journal of Medicine 219:471-474.
- Halbrecht J. (1939) Transfusion with placental blood. Lancet 2:202-203
- Halbrecht J (1939) Fresh and stored placental blood. Lancet 2:1263-1265.
- DeMarsh QB, Alt HL, Windle WF, Hillis DS (1941) The effect of depriving the
infant of its placental blood; on the blood picture during the first week of life.
JAMA 116:2568-2573.
- Wilson EE, Windle WF, Alt HL (1941) Deprivation of placental blood as a
cause of iron deficiency in infants. Am J Dis Child 62:320-327.
- DeMarsh QB, Windle WF, Alt HL (1942) Blood volume of newborn infant in
relation to early and late clamping of umbilical cord. Am J Dis Child 63:1123-
1129.
- Price EW (1944) Why tie the cord? British Medical Journal 1944, June 3, p
772.
- Vaughan, K (1944) Why tie the cord? British Medical Journal 1944, July 8, p
58.
- Chesterman CC (1944) Why tie the cord? British Medical Journal 1944, July
22, p 125.
- Jackson GA (1944) Why tie the cord? British Medical Journal 1944, July 22, p
125.
- Ballentine GN (1947) Delayed ligation of the umbilical cord. The Pennsylvania
Medical Journal 1947,Apr;50 (7):726-728.
- Landau DB, Goodrich HB, Francka WF, Burns FR (1950) Death of cesarean
infants: a theory as to its cause and a method of prevention. Journal of
Pediatrics 36:421-426.
- Colozzi AE (1954) Clamping of the umbilical cord; its effect on the placental
transfusion. N Engl J Med. 1954 Apr 15;250(15):629-32.
- Hormann G, Lemtis I (1954) Untersuchungen uber den fetalen
Plazentakreislauf warhrend der Nachgeburtsperiode. Zentralblatt fur
Gynakologie 76(9):329-341.
- Gunther M (1957) The transfer of blood between baby and placenta in the
minutes after birth. Lancet. 1957 Jun 22;272(6982):1277-80.
- Mahaffey LW, Rossdale PD (1957) On the newborn infant's oxygen supply.
Lancet 1957 Jul 13, ii:95.
- Jaykka S (1957) Capillary erection and lung expansion; an experimental study
of the effect of liquid pressure applied to the capillary network of excised fetal
lungs. Acta Paediatr. 1957 Jan;46(suppl 112):1-91.
- Whipple GA, Sisson TRC, Lund CJ (1957) Delayed ligation of the umbilical
cord; its influence on the blood volume of the newborn. Obstetrics and
Gynecology 10:603-610.
- Jäykkä, S (1958) Capillary erection and the structural appearance of fetal and
neonatal lungs. Acta Pædiatrica 47:484-500.
- Burnard ED (1959) The cardiac murmur in relation to symptoms in the
newborn. British Medical Journal (Jan 17):134-138.
- Leak WN (1959) When to tie the cord [letter]. British Medical Journal (Feb 28):
584.
- Mahaffey LW, Rossdale PD (1959) A convulsive syndrome in newborn foals
resembling pulmonary syndrome in the newborn infant. Lancet. 1959 Jun 13;1
(7085):1223-5.
- Desmond MM, Kay JL, Megarity AL (1959) The phases of "transitional
distress" occurring in neonates in association with prolonged postnatal
umbilical cord pulsations. Journal of Pediatrics 55:131-151.
- James LS. Physiology of respiration in newborn infants and in the respiratory
distress syndrome. Pediatrics. 1959 Dec;24:1069-101.
- Taylor PM, Egan TJ, Birchard EL, Bright NH, Wolfson JH (1961) Venous
hypertension in the newborn infant associated with delayed clamping of the
umbilical cord Acta Paediatrica 50:149-159
- Anonymous editorial [no authors listed] (1962) Placental transfusion. Lancet
1962 (Jun 9):1222-1223.
- Bound JP, Harvey PW, Bagshaw HB (1962) Prevention of pulmonary
syndrome of the newborn. Lancet. 1962 Jun 9;1:1200-3.
- Secher O, Karlberg P (1962) Placental blood-transfusion for newborns
delivered by Caesarean section. Lancet 1:1203-1205.
- Taylor PM, Bright NH, Birchard EL. Effect of early versus delayed clamping of
the umbilical cord on the clinical condition of the newborn infant. Am J Obstet
Gynecol. 1963 Aug 1;86:893-898.
- Gilles FH (1963) Selective symmetrical neuronal necrosis of certain brain stem
tegmental nuclei in temporary cardiac standstill. J Neuropathol Exp Neurol
1963;22:318, [abstract].
- Redmond A, Isana S, Ingall D. (1965) Relation of onset of respiration to
placental transfusion. Lancet. 1965 Feb 6;17:283-5.
- Anonymous editorial [No authors listed] A parting gift. Lancet. 1967 Jan 28;1
(7483):201-2
- Gilles FH (1969) Hypotensive brain stem necrosis: selective symmetrical
necrosis of tegmental neuronal aggregates following cardiac arrest. Archives
of Pathology 88:32-41.
- Myers RE (1972) Two patterns of perinatal brain damage and their conditions
of occurrence. American Journal of Obstetrics and Gynecology 112:246-276.
- Norman MG (1972) Antenatal neuronal loss and gliosis of the reticular
formation, thalamus, and hypothalamus. A report of three cases. Neurology
(Minneapolis) 22:910-916.
- Dunn PM (1972) Human "barkers". Equine Vet J. 1972 Jul;4(3):128-34.
- Griffiths AD, Laurence KM (1974) The effect of hypoxia and hypoglycemia on
the brain of the newborn human infant. Developmental Medicine and Child
Neurology 16:308-319.
- Grunnet ML, Curless RG, Bray PF, Jung AL (1974) Brain changes in
newborns from an intensive care unit. Developmental Medicine and Child
Neurology 16:320-328.
- Schneider H, Ballowitz L, Schachinger H, Hanefield F, Droeszus J-U (1975)
Anoxic encephalopathy with predominant involvement of basal ganglia, brain
stem, and spinal cord in the perinatal period. Acta Neuropathologica (Berlin)
32:287-298.
- Palmer AC, Rossdale PD. (1975) Neuropathology of the convulsive foal
syndrome. J Reprod Fertil Suppl. 1975 Oct;(23):691-4.
- Palmer AC, Rossdale PD. (1976) Neuropathological changes associated with
the neonatal maladjustment syndrome in the thoroughbred foal. Res Vet Sci.
1976 May;20(3):267-75.
- Leech RW, Alvord EC (1977) Anoxic-ischemic encephalopathy in the human
neonatal period, the significance of brain stem involvement. Archives of
Neurology 34:109-113.
- Roland EH, Hill A, Norman MG, Flodmark O, MacNab AJ (1988) Selective
brainstem injury in an asphyxiated newborn. Annals of Neurology 23:89-92.
- Natsume J, Watanabe K, Kuno K, Hayakawa F, Hashizume Y (1995) Clinical,
neurophysiologic, and neuropathological features of an infant with brain
damage of total asphyxia type (Myers). Pediatric Neurology 13:61-64.
- ...
More to be added to this bibliography. What an outrage that the evidence available
in the medical literature is so completely overlooked in recent research reports.
3 May 07 - IMFAR, Seattle - research on perception of syllables in noise
Auditory impairments in autism are being recognized more and more. I especially
liked a presentation today by a young scholar from Holland, Wouter Bastiaan Groen.
I asked him later if he knew the research of Michael Church with fetal alcohol
children, and diminished perception of words in background noise. That was back in
the 1980s. "No I was around five years old then." Groen reported on his research
comparing autistic with normal children on the ability to detect speech in noise. The
children with autism were impaired compared with control children.
Groen compared his work to that on visual perception in autism, and theories of lack
of central coherence in autism. He described lack of ability to "dis-embed" words
from background noise as a manifestation of cortical "under-connectivity" in
individuals with autism. My thinking was that it more likely revealed an inability to
detect syllabic features enroute to the cortex, in the brainstem (the inferior colliculi in
particular). I had my hand up, but instead an old curmudgeon got up and told the
young presenter he thought his interpretation of his data was far-fetched.
I spoke with young Groen (and a colleague) later, and congratulated him on a nice
piece of research. I told him I will have a poster up tomorrow, which may have some
bearing on why children with autism may have problems hearing syllables in
background noise. I am so glad to see research like this being done.
4 May 07 - Notes on testing of children with fetal alcohol syndrome (FAS)
I happen to have notes in my computer on autism in fetal alcohol syndrome, and the
tests used by Church et al. (1997) to assess hearing and language perception.
Church et al. studied 22 FAS children with a special focus on hearing and
developmental language problems. Conductive hearing loss due to recurrent
serous otitis media occurred in 17 children, and 6 children had measurable
sensorineural hearing loss. Two of the children with conductive hearing loss
exhibited echolalia, repetitive play, and self-stimulating behaviors which Church et al.
termed autistic tendencies. Twelve subjects could be tested for central auditory
processing deficits, and all were classified as abnormal.
The tests used for assessment of hearing and language disorders by Church et al.
could possibly be employed to gain better insight into the hearing and language
impairments of children with autism. The two children with fetal alcohol syndrome
and autistic tendencies in their study could not be tested on the word and sentence
recognition tasks. However, higher functioning children with autism might be
expected to cooperate in attempting these listening tasks. Two of the tests
employed by Church et al. involved word recognition in quiet (WRIQ) or with
competing noise, word recognition in ipsilateral noise (WRIN).
The competing sentence test (CST) requires reporting content of two different 6 to 7
word sentences presented simultaneously to each ear (Willeford, 1985). As
described by Church et al., the word recognition in noise (WRIN) test is a figure-
ground test that assesses the subject's ability to identify words in the presence of
background noise. Signal extraction from noise is believed to be one of the primary
functions of the inferior colliculus. Thus the WRIN test, or modifications of it for non-
verbal children, might be as valuable as auditory evoked potentials in assessing
impairment of the auditory pathway at this level.
The children in Church et al.’s study were patients at a craniofacial-anomalies and
cleft palate clinic; twelve of the 22 children studied had cleft palate, including the two
children who displayed autistic behaviors. Fifteen of the children had serious dental
anomalies with misalignment of the jaws. Anomalies of outer ears and eyes were
apparent in many, as well as skeletal and internal organ malformations.
Most children with autism do not have physical anomalies. Kemper and Bauman
(1998) made special note of this as part of the clinical background of their subjects.
Kemper and Bauman suggested some event around 30 weeks of gestation might
interfere with brain development and cause the pattern of pathology they observed.
Rodier et al. (1997) investigated malformations as part of a study of children with
autism in Nova Scotia, but they found only minor deviations. Autistic children with
physical deformities more likely represent those with autistic behaviors
accompanying disorders caused by exposure to teratogenic substances during
gestation, including alcohol.
Well formed facial features indicates that impairment of the brain in the core
syndrome of autism occurs late in gestation, in the perinatal period, or during the
first few months of life, rather than at early stages of tissue differentiation. This is far
different from fetal alcohol syndrome, where the developing fetus may be repeatedly
subjected to toxic injury throughout pregnancy. The finding of children with autistic
behaviors among those with FAS is of interest however because it means the brain
areas impaired in autism are among those also affected by prenatal alcohol
exposure in some cases.
Church MW, Eldis F, Blakley BW, Bawle EV (1997) Hearing, language, speech,
vestibular, and dentofacial disorders in fetal alcohol syndrome. Alcoholism, Clinical
and Experimental Research 21:227-237.
Willeford JA (1985) Sentence tests of central auditory dysfunction, in Katz J, ed,
Handbook of Clinical Audiology. Baltimore: Williams & Wilkins. Countway Library of
Medicine WV 270.3 H2363 1985.
Kemper TL, Bauman M (1998). Neuropathology of infantile autism. Journal of
Neuropathology and Experimental Neurology 57:645-652.
Rodier PM, Bryson SE, Welch JP (1997) Minor malformations and physical
measurements in autism: data from Nova Scotia. Teratology 55:319-325.
5 May 07 - IMFAR highlights
May 4:
Peter Bell, Autism Speaks - "Let's figure this thing out so we can find a cure."
Patricia Kuhl - Language learning and the social brain
Timothy Buie -
Increased prevalence of Crohn's disease, asthma, type I diabetes, and obesity as
well as autism, and previously discussed at the Current Trends in Autism (CTIA)
conference, March 23.
Tom Insel, NIMH -
http://www.nimh.nih.gov/autismiacc/index.cfm
May 5:
Cure Autism Now (CAN), founding parents
Portia Iversen -
Son now 15, need for more research on children who can't speak, or use language
for communication. Need to keep track of the history of research.
Jon Shestack -
Ten to twelve years ago, no internet, no community when CAN formed. More
sadness now, not less. Need for more relevant research, less on eye-tracking and
face-processing. We have not come as far as we should. This is a big problem, with
a need for constant challenge. We need to push harder for things that will really
advance the field. Now we face long-term care worries. Involve parents. "Nobody
knows our kids better than we do," but some scientists have never seen a kid with
autism.
Diffusion Tensor Imaging (DTI)
Marco Catani -
History - Wernicke to Norman Geschwind and disconnection syndromes.
Autism and language pathways, Wernicke to Broca, and a third projection found with
DTI - proposed by Norman Geschwind.
Age related changes of lateralization of perisylvian networks, and they continue
developing past childhood, except in subjects with Asperger syndrome.
Catani M. Diffusion tensor magnetic resonance imaging tractography in cognitive
disorders. Curr Opin Neurol. 2006 Dec;19(6):599-606.
Catani M, ffytche DH.The rises and falls of disconnection syndromes.
Brain. 2005 Oct;128(Pt 10):2224-39.
Catani M, Jones DK, ffytche DH.Perisylvian language networks of the human brain.
Ann Neurol. 2005 Jan;57(1):8-16.
6 May 07 - IMFAR reflections
I read the abstracts for poster sessions 5 and 6 on the flight home today, between
looking out the window at the spectacular views below. The comments of the
parents who spoke, and with whom I spoke, echoed in my head, "We need to figure
this thing out and find a cure," "We need more relevant research, and less on things
like abnormal eye tracking and face processing, "We need more involvement of
parents, because nobody knows our kids better than we do," "We need more
research on severely impaired children with little or no speech," and I especially liked
Portia Iversen's idea that we need to keep track of the history of research.
If the increased prevalence of autism is due to "diagnostic substitution," what
information do we have from doctors who cared for patients in the past under
another diagnostic label? In fact, I want to add this to my to-do list.
Reflecting on the movie we were shown, "Autism Every Day," I have to count my
blessings that neither Conrad or Ralf ever had behavioral problems as serious as
parents were coping with in that film. Potty training was not a problem, nor was joint
attention, and when Conrad thought I was sad, he would bring me a kleenex, and to
me that represents "theory of mind" with a great deal of empathy.
The children in that film clearly displayed autistic behaviors, but they appeared more
cognitively impaired than the condition described by Kanner.
The plane came into Boston from the north, then out to sea, then south over the
harbor islands, Boston Light, Hull with its two beautiful windmills, then west over
Quincy; and out my window I saw Ralf's house just beyond the Fore River Bridge. I
was so excited, I took my phone out of my bag and turned it on as soon as we were
told we could. I called Ralf. "Where are you?" he asked.
"We just landed," I said, "And, did you see the plane fly just beyond the Fore River
Bridge at five past five?"
"Yes, I did, and I wondered if it was your plane. But it wasn't a 747."
"No, it's a brand new Boeing 737 - wait a minute," I pulled the card out of the seat
back (and have already forgotten the model of the plane). Ralf recognized the
model, because planes, trains, and cars are among his special interests. I told him
the bus to the airport this morning went right past Boeing Field in Seattle, and he
told me he had watched a documentary on TV a few months ago about test flights
from that field.
I am so grateful I can have this kind of conversation with Ralf, and over the phone.
Conrad was never able to talk over the phone. Conrad could hear, and remember
long sequences of music and speech. He just never learned to make sense out of
what he heard any more than I can make sense out of what people speaking a
foreign language are saying. I am very limited even in understanding people
speaking those languages I learned in school.
Patricia Kuhl's talk was on how infants younger than six months of age are citizens of
the world - they are able to learn any language they hear, and without accent. This
ability declines over the first decade of life as a child perfects proficiency in the
mother-tongue. Somehow, children with autism miss the "citizen of the world" stage
of development. Conrad could hear, but was as if deaf when it came to
comprehending speech.
7 May 07 - More reflections: A cure for autism? Early auditory testing?
Today was the first day of a big biotech convention taking place in Boston this week,
and I heard on the news that Michael J. Fox addressed the attendees with some
anger about the slow progress being made to find a cure for Parkinsonism. This is
reminiscent of some of the anger expressed by parents of children with autism at
IMFAR, and that perhaps too much research is done trying to define characteristics
of autism that parents are already too well aware of.
What would be most useful? I think most of us would like to find a way to help our
children develop normal language.
According to Patricia Kuhl, the first six months of life may be the most critical period
for a child to gain familiarity with the distinctive sound patterns of their native
language. The experiment she showed was dramatic, of a baby playing with a toy,
ignoring a repetitive vowel sound to one side, but with sudden orientation to the side
of the sound source when it changed to another vowel. Perhaps this is the test that
should be standard for all babies in the first month or two of life, and if orientation to
a novel vowel sound does not cause orientation, special methods to teach language
should be started. Perhaps the young infant who does not orient to a novel vowel
sound should begin being taught as if deaf.
Children with autism are not deaf, but hypersensitivity to some sounds and failure to
orient to others indicates distortion of what is heard that interferes with detection of
vowels, syllable boundaries, and other distinctive features of spoken language. At
IMFAR there were papers describing abnormal prosody of speech produced by
some (if not most) children with autism - distortion of speech reminiscent of that of
deaf children and adults.
A cure for autism will come only when function can be restored to damaged neurons,
and at least some of these neurons will likely be found in the auditory pathway. For
deaf children cochlear implants come close to being a cure. In autism, the problem
is not in the ear or cochlear nucleus. The inferior colliculi in the midbrain auditory
pathway are likely to be affected in autism, and I will continue to try to attract
attention to investigating this possibility - until someone can produce positive
evidence that there is no impairment of function in the inferior colliculi. I have posted
a proposal for using fMRI to look for functional status in the inferior colliculi at
http://www.inferiorcolliculus.org/presentation.html. So far, I have not been able to
find anyone interested in doing research of this kind, but I plan to try to contact
some of the people who presented fMRI findings at IMFAR.
10 May 07 - Inferior colliculus, MRI investigation of perinatal myelination
This morning in PubMed:
Sano M, Kaga K, Kuan CC, Ino K, Mima K. Early myelination patterns in the
brainstem auditory nuclei and pathway: MRI evaluation study.
Int J Pediatr Otorhinolaryngol. 2007 May 5; [Epub ahead of print]
I was able to obtain the full text of this in-press paper. Of interest are the citations to
older histological research on myelination. The 1920 book by Flechsig is new to me,
but the paper by Langworthy (1933) is not mentioned. MRI shows that the time-
course of myelination is somewhat later than shown in the histological studies. An
excellent explanation is given of events that occur during myelin formation.
Comparisons are made of myelination and development of auditory evoked
potentials.
Histological references:
[1] P. Flechsig, Anatomie des Menschichen Gehirn und Rueckenmarks
auf Myelogenetischer Grundlage, Thime, Leipzig, 1920.
[2] P.I. Yakovlev, A. Lecours, The myelogenetic cycles of regional maturation of the
brain, in: Minkowski (Ed.), Regional Development of the Brain in Early Life, Blackwell
Scientific Publication, Oxford, 1967, pp. 3—70.
[3] L.B. Rorke, H.E. Riggs, Myelination of the Brain in the Newborn, Lippincott
Company, Philadelphia, 1969.
[4] J.K. Moore, L.M. Perazzo, A. Braun, Time course of axonal myelination in the
human brainstem auditory pathway, Hear Res. 87 (1/2) (1995) 21—31.
References on auditory evoked potentials:
[5] C.W. Ponton, J.J. Eggermont, S.G. Coupland, R. Winkelaar, The relation between
head size and auditory brainstem response interpeak latency maturation,
J. Acoust. Soc. Am. 94 (4) (1993) 2149—2158. More of interest in PubMed by these
authors.
[6] P.A. Despland, R. Galambos, The auditory brainstem response (ABR) is a useful
diagnostic tool in the intensive care nursery, Pediatr. Res. 14 (2) (1980) 154—158.
[7] A.G. Pettigrew, D.J. Henderson-Smart, D.A. Edwards, Evoked potentials and
functional development of the auditory system, in: M. Rowe, L. Aitkin (Eds.),
Information Processing in Mammalian Auditory and Tactile Systems, Alan R. Liss,
Inc., New York, 1990, pp. 295—308.
Comparisons of T1- and T2-weighted images:
With the progress of myelination, the signal intensity of MRI changes from low to
high on T1-weighted imaging and from high to low on T2- weighted imaging [24—
28]. p2
References on MRI of the auditory pathway:
[24] J.A. Stone, D.W. Chakeres, P. Schmalbrock, High-resolution MR imaging of the
auditory pathway, Magn. Reson. Imag. Clin. N. Am. 6 (1) (1998) 195—217.
[25] D. Bergerbest, D.G. Ghahremani, D.E. Gabrieli, Neural correlates of auditory
repetition priming: reduced fMRI activation in the auditory cortex, J. Cogn. Neurosci.
16 (2004) 966—977.
[26] K. Hittmair, D. Wimberger, T. Rand, L. Prayer, G. Bernert, J. Kramer, et al., MR
assessment of brain maturation: comparison of sequences, Am. J. Neuroradiol. 15
(1994) 425—433.
[27] B.D. Flannigan,W.G. Bradley Jr., J.C. Mazziotta,W. Rauschning, J.R. Bentson, R.
B. Lufkin, G.B. Hieshima, Magnetic resonance imaging of the brainstem: normal
structure and basic functional anatomy, Radiology 154 (2) (1985) 375—383.
[28] J.T. Curnes, P.C. Burger, W.T. Djang, O.B. Boyko, MR imaging of compact white
matter pathways, Am. J. Neuroradiol. 9 (6) (1988) 1061—1068
Excerpts from methods:
patients underwent MRI because a brain disorder was suspected. Images
demonstrating anomalies, infarcts, or hemorrhages in the brainstem were excluded
from the study. No brainstem lesions or severe central nervous system malformation
were apparent in any subject of this study.
The present study examined 1536 magnetic resonance images (192 cases with
eight slices each by T1- and T2-weighted imaging) and analyzed the progress
patterns of myelination at four different checking points (cochlear nucleus, superior
olivary nucleus, lateral lemniscus, and inferior colliculus) according to region-of-
interest (ROI)- based analysis.
Reference on fetal brain development:
[29] A. Fee-Higins, J.C. Larroche, Development of the Human Foetal Brain, INSERM
Masson, Paris, 1987.
Excerpts from the discussion:
ABR studies indicate that the speed of axonal conduction is low in children under 1
year of age and rapid axonal conduction gradually develops in the brainstem
auditory nuclei and pathways. The increase of myelin density is likely to be a factor
in the steady decrease in ABR interval between wave I and waves III—V. p9
Myelination does not take place suddenly but happens gradually, so definite
myelination, with a full change of myelin sheath ingredients (loss of water and gain of
lipids), is needed to be detectable by MRI. This study shows the progress pattern
of myelination in the brainstem auditory nuclei and pathway on MRI. These results
can be used to assess with MRI the auditory system maturation of infants. p10
Inferior colliculi on MRI image:
15 May 07 - Inferior colliculus, cytochrome oxidase activity in mutant mice
New in PubMed this morning:
Hayzoun K, Lalonde R, Mariani J, Strazielle C. Regional variations of cytochrome
oxidase activity in the central auditory system of Reln(rl-Orl) (reeler) mutant mice.
Neurosci Res. 2007 Apr 20; [Epub ahead of print].
Use of radioactive tracers revealed that blood flow and glucose utilization are
greater in the inferior colliculi than in any other part of the brain (see references,
data, and discussion at: http://www.conradsimon.org/InferiorColliculus.shtml). The
deoxyglucose method for measuring glucose utilization was used to investigate
metabolic maturation of the brain in neonatal cats by Chugani et al. (1991) who
found, as in other studies using the deoxyglucose method, that uptake was highest
in the inferior colliculus. As continuation of the same study of metabolic maturation,
Hovda et al. (1992) investigated distribution of cytochrome oxidase in developing
cats.
Cytochrome oxidase is a mitochondrial enzyme that activates oxygen in the final step
of the aerobic metabolic pathway. Hovda et al. made special note of the high
oxidative capacity of the inferior colliculus, which was 25 percent higher than other
brainstem structures seven days after birth. As in the deoxyglucose uptake studies,
cytochrome oxidase levels exceeded adult levels in several brain structures. Hovda
et al. commented on the development of deoxyglucose uptake in relation to the
development of cytochrome oxidase. Cytochrome oxidase can be an indicator of
capacity for aerobic metabolism. The finding by Chugani et al. of a developmental
pattern of glucose uptake that parallels development of cytochrome oxidase ensures
that glucose does not enter the brain until it can be metabolized in the aerobic
pathway.
The paper by Hayzoun et al. reports differences from normal in cytochrome oxidase
enzyme distribution in the auditory system of mice with a mutation in the "RELN
gene." This gene has been implicated in some cases of autism (Fatemi et al. 2005),
who described mutant mice as ataxic, with a "reeling gait," and with abnormalities in
orientation of neurons in the cortex and cerebellum of the brain. Fatemi et al. found
postmortem reductions of Reelin gene expression in the cortex (frontal and parietal
lobes) and cerebellum in brain tissue from individuals who were autistic during life.
Fatemi et al. did not look at tissue from the auditory cortex or brainstem.
Hayzoun et al. report cytochrome oxidase (CO) activity in the mutant mice that is
lower in some auditory structures and higher in others. In the dorsal cochlear
nucleus (DCN) a significant decrease was found in the superficial layer, and
significant increase in the granule cell layer. Decreased activity was also found in
an area ventral to the superior olive, but activity was significantly increased in
several other structures and especially in the inferior colliculus.
Hayzoun et al. also noted abnormalities in cell orientation as described by Fatemi et
al. but only discussed the patterns of cytochrome oxidase as altered, and reflective
perhaps of the complexitiy of descending as well as ascending pathways in the
auditory system.
This is an article "in press," which I am fortunate to be able to access in advance
through my husband's academic connections. The pictures of the auditory
structures from cochlear nucleus to cortex are most interesting, and of course for
me, gazing at the inferior colliculus holds the greatest fascination. I plan to request
permission for posting their pictures on this blog site, but can't resist a sneak
preview:
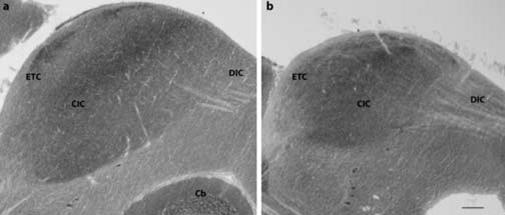
Fig 4. CO labelling in inferior colliculus of control (a) and Relnrl-Orl (b) mice. Among
the different central (CIC), dorsal (DIC), and external (EIC) subregions of inferior
colliculus, CO labelling is heterogeneous in the control mouse; in the Relnrl-Orl
mutant, the higher CO labelling in dorsal and central nuclei yields a homogeneous
staining to this region. The atrophied Relnrl-Orl cerebellar vermal cortex (Cb) is not
visible at this frontal plane. Scale bar = 100 μm. The plane of section passes at 1.54
mm posterior to the interaural plane of reference in control mouse. (from Hayzoun K.
et al. (2007).
References:
- Hayzoun K, Lalonde R, Mariani J, Strazielle C. Regional variations of
cytochrome oxidase activity in the central auditory system of Reln(rl-Orl)
(reeler) mutant mice. Neurosci Res. 2007 Apr 20; [Epub ahead of print].
- Chugani HT, Hovda DA, Villablanca JR, Phelps ME, Xu WF. Metabolic
maturation of the brain: a study of local cerebral glucose utilization in the
developing cat. J Cereb Blood Flow Metab. 1991 Jan;11(1):35-47.
- Hovda DA, Chugani HT, Villablanca JR, Badie B, Sutton RL. Maturation of
cerebral oxidative metabolism in the cat: a cytochrome oxidase
histochemistry study. J Cereb Blood Flow Metab. 1992 Nov;12(6):1039-48.
- Fatemi SH, Snow AV, Stary JM, Araghi-Niknam M, Reutiman TJ, Lee S,
Brooks AI, Pearce DA. Reelin signaling is impaired in autism. Biol
Psychiatry. 2005 Apr 1;57(7):777-87.
17 May 07 - Milieu research - seizure disorder
Many of the patients at Bridgewater State Hospital are given medications to control
seizures. I remember back in the 1970s, when we were lobbying hard for special
education, the campaign for "community care" and de-institutionalization were well
underway. I never had any awareness of these issues until I had a child whose
education and future were involved. I remember one doctor who got up at several
meetings on hospital closures, and who proclaimed that state hospitals were first
built to care for epileptics. Now, he assured us, epilepsy is controlled by medications.
Three and a half decades later, we provide care for epileptics who have come to the
attention of the police, in the community. Often, in the community, they do not take
the medications prescribed to control seizures, nor do they see a doctor often
enough for medication changes to manage more frequent seizures or minimize side
effects. One such patient went into a prolonged seizure state today, and an
ambulance had to be called to take him to the hospital. This is the same patient for
whom I had to fax parts of his medical record up to the Beth Israel Hospital - two
months ago, on a snowy evacuation day holiday.
This patient, now in his early fifties, was hospitalized in his teens at the old Boston
State Hospital, which was one of the first state hospitals to be closed. Has this
patient's journey back into the community, and into trouble with the law, then into the
correctional system benefited him?
The state hospitals were referred to as asylums when they were first built. Asylum
has been totally denied patients like the one we sent out in an ambulance today.
Beth Israel is the number one hospital for neurology in the world. If they needed
information sent, the local hospital where he was sent today should also need more
information. Wouldn't it have been better for this patient to have had lifelong
residency in Boston State Hospital? Now his care is fragmented, and needed
information pieced together as he moves from one facility to another.
We have medications for seizure disorders, but they are not perfect, and certainly
are not cures anymore than are any of the anti-psychotic pills that we give out in
such large numbers. Presumptions that people with mental illnesses are better
cared for in the community are wrong. It may, in the long run, cost even more than if
the state hospitals had been retained.
18 May 07 - My son the savant
Ralf and I get together about once a week, usually on Fridays to go to the library
and work on topics in the GED book (Princeton Review) that I got for him.
Afterwards we take a walk around Quincy Center, and usually visit two of his favorite
hobby shops. Last week I balked at the idea I might chip in some money to
purchase something that caught his fancy. "No, because I went to Seattle, I won't be
getting enough money in my next paycheck for frivolous expenditures."
When I arrived at his house today, he had $15.77 in an envelope, from his account
at the house (money from Social Security). I was told they needed a receipt for
whatever he bought with the money.
At the store he carefully examined several model cars, then picked three and said, "I
think these come to just under 15 dollars -- So with tax, my $15.77 should cover it."
"Wow, you're quick with numbers," the owner of the store said.
"I know," Ralf replied, and yes numbers have always been one of his strengths.
The clerk who had taken the selection of cars out of the display case for Ralf to look
over, then made out a receipt, by hand, and took quite a bit of time figuring out the
exact tax.
On the way home we discussed what he had been working on for the GED, and he
told me he is now starting to work on the reading and writing sections. These are
two more of his strengths, and I suggested he should maybe try to write small
summaries of some of his memories growing up -- not more than a page or so. I
suggested to him that quite a few books have come out lately, written by people with
Asperger syndrome, and that many people have found these quite interesting.
People want to try to figure out how people with problems overcome them.
"You might even be able to make some money from writing a book," I suggested,
and that idea seemed to appeal to him. Once again, I suggested no more than a
page for memories of Ward Six, Gaebler School, the Cambridge YMCA, summers at
Camp Massapoag, then Riverview. He seemed interested. I look forward to seeing
what he may produce.
19 May 07 - Rise in autism prevalence, news article in BMJ
Hitchen L. Rise in prevalence of autism in children continues to baffle researchers.
BMJ. 2007 May 19;334(7602):1027 [no abstract].
News report on a conference in England. Professor Tony Charmin discussed his
previously published research:
Baird G, Simonoff E, Pickles A, Chandler S, Loucas T, Meldrum D, Charman
T.Prevalence of disorders of the autism spectrum in a population cohort of children
in South Thames: the Special Needs and Autism Project (SNAP). Lancet. 2006 Jul
15;368(9531):210-5.
Charman commented that the prevalence statistics might change as some children
(with no biological or genetic markers for the disorder) grow older and no longer
display autistic behaviors. "It might be that such people will no longer be classed as
having the disorder, which could lead to a fall in prevalence."
He did acknowledge the "difficulties" faced by children with autism, and their parents.
One rapid response, from Dr. A. Breck McKay in Brisbane Australia, suggests a
problem with orientation related to midbrain dysfunction. I just submitted my own
response.
20 May 07 - Milieu research, memories & reflections
Coming home after forced overtime, tired and even ready to quit, I have recently felt
no desire to think about the milieu at work. Yesterday, I was quickly rescheduled to
work on my old "penthouse unit" for men mostly serving life sentences - 54 men to
get 8am medications ready for in an hour and a half. Once meds were taken care
of, I was in the milieu again that for many years I found so fascinating.
Going to breakfast, patients from another building were in the lobby waiting to leave.
So many I have known for more than 15 years now, heard their stories and their
struggles.
"Where've you been?"
"Mostly in the infirmary." I mostly work with men there with chronic health problems,
and, except for codes, rarely leave the medical building.
One young man, came up and excitedly explained that he is scheduled to go to a
DMH hospital soon. I hope so, and hope he will not be put out into a community
group home too soon.
In the chow hall, the downstairs unit from our building was already nearly finished
eating. I noticed the young man from Westborough who had a bad med reaction a
few weeks back. He looks wonderful now. He spoke to me on the way out - he had
taken the juice pitcher by mistake with his tray, and returned to put it back on the
table.
"I can't believe I walked off with the pitcher," he said.
I asked him if he remembered the patient a few years back who came into the chow
hall on a hot summer day, and picked up the pitcher and drank from it before taking
his seat.
"I remember that - of course."
I am glad to see this young man looking so well. I hope I get assigned out of the
infirmary more often. I'm feeling more motivated to keep going to work.
The rapid-response I submitted to the BMJ last evening is already posted!
22 May 07 - Milieu research, bad behavior in court
On my way home yesterday, I heard a brief news report on the radio that one of our
former patients had exhibited some outrageous behavior in court. This morning it
was in the newspaper. He somehow was able to punch one of the jurors down to the
floor. I guess this isn't as bad as the time an inmate attacked his lawyer in court. --
an inmate I didn't know. They are sent to Bridgewater for evaluation of competency
to stand trial. How the patient in the paper today could have been found competent
for much of anything is a mystery to me. He is one of those I thought would not
really pass the Turing Test. He might seem to make sense in a few minutes of
conversation, but his daffiness became evident over the course of repeated day by
day interactions in the milieu. Lashing out and hitting another person is a very
retarded thing to do -- sometimes referred to as "dumb strength" among my
coworkers. Later news report on the radio that a mistrial has been declared.
25-26 May 07 - The inferior colliculus, research of Marcus Lira Brandão
In progress -- I cited the paper by Brandão et al. (1993) in my viewpoint paper in
2000 (http://www.conradsimon.org/WorkingPaper.shtml) as providing evidence of the
inferior colliculi as an alerting center for the brain (section 9). In section 15, I
discussed experiments by Denny-Brown (1962), Sprague et al. (1961), and Jane et
al. (1965) that suggested the midbrain tectum, lateral lemniscal tracts, and inferior
colliculi were important for general awareness. The papers from Brandão's lab
appear to be important sources for neuroanatomical and neurochemical substrates
of awareness, alerting, consciousness provided by the inferior colliculi as a vigilance
center of the brain.
- Ferreira-Netto C, Borelli KG, Brandao ML. Distinct Fos expression in the brain
following freezing behavior elicited by stimulation with NMDA of the ventral or
dorsal inferior colliculus. Exp Neurol. 2007 Apr;204(2):693-704.
- Brandao ML, Borelli KG, Nobre MJ, Santos JM, Albrechet-Souza L, Oliveira
AR, Martinez RC. Gabaergic regulation of the neural organization of fear in
the midbrain tectum. Neurosci Biobehav Rev. 2005;29(8):1299-311.
- Brandao ML, Troncoso AC, de Souza Silva MA, Huston JP. The relevance of
neuronal substrates of defense in the midbrain tectum to anxiety and stress:
empirical and conceptual considerations. Eur J Pharmacol. 2003 Feb 28;463
(1-3):225-33.
- Brandao ML, Coimbra NC, Osaki MY. Changes in the auditory-evoked
potentials induced by fear-evoking stimulations. Physiol Behav. 2001 Feb;72
(3):365-72.
- Cuadra G, Zurita A, Macedo CE, Molina VA, Brandao ML. Electrical stimulation
of the midbrain tectum enhances dopamine release in the frontal cortex. Brain
Res Bull. 2000 Jul 15;52(5):413-8.
- Brandao ML, Anseloni VZ, Pandossio JE, De Araujo JE, Castilho VM.
Neurochemical mechanisms of the defensive behavior in the dorsal midbrain.
Neurosci Biobehav Rev. 1999;23(6):863-75.
- Brandao ML, Melo LL, Cardoso SH. Mechanisms of defense in the inferior
colliculus. Behav Brain Res. 1993 Dec 20;58(1-2):49-55.
- Schmitt P, Carrive P, Di Scala G, Jenck F, Brandao M, Bagri A, Moreau JL,
Sandner G. A neuropharmacological study of the periventricular neural
substrate involved in flight. Behav Brain Res. 1986 Nov;22(2):181-90.
27 May 07 - Outcome studies - Charman et al. (2005)
In progress -- Rapid responses to Hitchen L. Rise in prevalence of autism in
children continues to baffle researchers. BMJ. 2007 May 19;334(7602):1027,
include two from me, the first in response (in part) to the first rapid response
suggesting a midbrain cause for impaired orientation reactions in autism. The
second in response to Dr. Hutcheon, and obstetrician who opposes umbilical cord
clamping at birth.
The full text of the news report suggests that prevalence statistics may change as
children with autism grow up and outgrow the diagnosis of autism - this from Prof.
Charman, but then I found an article by him that found of 26 children followed to age
seven, 22 remained autistic. I may try corresponding with him.
Prevalence investigations must begin to question what systems of the brain are
affected, and how these impairments come about.
--
Charman T, Taylor E, Drew A, Cockerill H, Brown JA, Baird G. Outcome at 7 years of
children diagnosed with autism at age 2: predictive validity of assessments
conducted at 2 and 3 years of age and pattern of symptom change over time.
J Child Psychol Psychiatry. 2005 May;46(5):500-13.
28 May 07 - Evidence gathered in the process of reinventing the wheel
Article attached to email from a friend this morning:
Zaramella P, Freato F, Quaresima V, Secchieri S, Milan A, Grisafi D, Chiandetti L.
Early versus late cord clamping: Effects on peripheral blood flow and cardiac
function in term infants. Early Hum Dev. 2007 May 18; [Epub ahead of print]
Excerpts:
"The current obstetric approach is to clamp the cord within the first 10–15 s
after birth," p2 of article in press.
"Cord clamping time seems to be particularly crucial to the baby's pulmonary
adaptation to extrauterine life," p2 of article in press.
"Eleven early-clamped newborn infants (at 30 s) were compared with 11
late- clamped babies (at 4 min). They were enrolled by a physician taking
part in the research, who decided the clamping time at random (not based
on any clinical indication) and timed cord clamping with a stopwatch."
"Newborn infants delivered vaginally in the late clamped group were held in
their mothers' arms while waiting supine for the cord to be clamped."
Apgar score ranges were not significantly different, but higher in late-
clamped group.
Early clamped: 1min (7-9) 5min (9-10)
Late clamped: 5min (9-10) 5min (10-10)
"Capillary hematocrit (Ht%) was measured on day 3 of life in blood drawn
from a heel-prick," p3.
Hematocrit (day 3)
Early clamped: 54 (range 50–62)
Late clamped: 62 (range 58–74)
"Echocardiography was performed on day 3 of life, prior to the NIRS
measurements, when the patent ductus arteriosus is assumed to have
closed in term infants," p3
"Our data confirm that late clamping is unassociated with any increased risk
of hyperbilirubinemia," p4.
Discussion: "Immediate cord clamping seems to be the most common
clamping practice, in spite of the lack of any randomized trials reporting any
negative side effects of late clamping in newborn infants."
"We also found no change in peripheral (leg) blood flow but a higher end
diastolic left ventricular diameter in the late-clamped infants, suggesting a
greater filling of the left ventricle with no increase in peripheral perfusion.
This result seems to contrast with a recent study on preterm vaginally
delivered newborns that demonstrated an increased volemia in late (median
time 90 s) clamped infants due to placental transfusion [37]. This
discrepancy may be related to a peripheral vasodilation in our healthy term
newborn infants, and thus have to do with a different gestational age:
placental transfusion seems to be more pronounced in lower gestational age
groups than in more mature infants [37]."
"Conclusion: Our results demonstrate that late cord clamping coincides with
a greater placental transfusion, expressed by an increase in hematocrit and
hemoglobin, and a larger left ventricle diameter at the end of the diastole
without any change in peripheral perfusion or oxygen metabolism. Late
clamping does not seem to increase the risk of jaundice, however. The
increased LVD(D) with no change in BF might improve the extrauterine
adaptation of newborn infants, mainly redistributing the capillary blood
toward alternative vascular beds, preventing a relative ischemia and
hypovolemia." p5.
Comment:
1. Most infants breathe immediately at birth, thus Apgar scores were only slightly
less than perfect in the infants subjected to immediate clamping in this small sample
of babies.
2. Peripheral perfusion was not found increased in the babies allowed a 4-minute
postnatal placental transfusion, and this was attributed to vasodilation.-- a healthy
response to increased blood flow.
3. References on time of cord clamping went back only as far as 1980 (Nelson NM
et al. A randomized clinical trial of the Leboyer approach to childbirth. N Engl J Med.
1980 Mar 20;302(12):655-60.). So much evidence had been gathered earlier that
demonstrated the advantages of allowing postnatal placental respiration.
4. From http://www.pregnancy-info.net/leboyer.html
Leboyer in the Delivery Room
While not everyone subscribes to the gentle leboyer birth technique, the method has had
some influence in delivery rooms. Many delivery rooms have tried to minimize the noise
levels to make the atmosphere more peaceful for mothers. Health care providers also
no longer smack babies when they are born to get them to breathe. Instead, many
babies are massaged to encourage their first breath before the umbilical cord is cut.