- Belmonte MK, Carper RA (2006) Monozygotic twins with Asperger syndrome: differences in
behaviour reflect variations in brain structure and function. Brain Cogn. 2006 Jun;61(1):110-
21.
- Greenberg DA, Hodge SE, Sowinski J, Nicoll D (2001) Excess of Twins among Affected
Sibling Pairs with Autism: Implications for the Etiology of Autism. American Journal of Human
Genetics 69:1062-1067.
- Norman MG (1982) Mechanisms of brain damage in twins. The Canadian journal of
neurological sciences 1982 Aug;9(3):339-44.
- Davis JO, Phelps JA, Bracha HS (1995) Prenatal development of monozygotic twins and
concordance for schizophrenia. Schizophrenia Bulletin 21:357-366. Published erratum
appears in Schizophrenia Bulletin 21:539.
- Lowe TL, Tanaka K, Seashore MR, Young JG, Cohen DJ (1980). Detection of phenylketonuria
in autistic and psychotic children. Journal of the American Medical Association 243:126-128.
- Williams RS, Hauser S, Purpura DP, deLong GR, Swisher CN (1980) Autism and mental
retardation: Neuropathologic studies performed in four retarded persons with autistic
behavior. Archives of Neurology 37:748-753.
- Chen CH, Hsiao KJ (1989) A Chinese classic phenylketonuria manifested as autism. British
Journal of Psychiatry 155:251-3
- Miladi N, Larnaout A, Kaabachi N, Helayem M, Ben Hamida M (1992) Phenylketonuria: an
underlying etiology of autistic syndrome. A case report. Journal of Child Neurology 7:22-23.
- Leuzzi V, Trasimeni G, Gualdi GF, Antonozzi I (1995) Biochemical, clinical and
neuroradiological (MRI) correlations in late-detected PKU patients. Journal of Inherited
Metabolic Disease 18:624-634.
- Gillberg C, Coleman M (1996). Autism and medical disorders: a review of the literature.
Developmental Medicine and Child Neurology 38:191-202.
- Migeon BR, Dunn MA, Thomas G, Schmeckpeper BJ, Naidu S (1995) Studies of X inactivation
and isodisomy in twins provide further evidence that the X chromosome is not involved in
Rett syndrome. Am J Hum Genet. 1995 Mar;56(3):647-53.
- Subramaniam B, Naidu S, Reiss AL (1997) Neuroanatomy in Rett syndrome: cerebral cortex
and posterior fossa. Neurology 48:399-407.
- Feekery C, Parry-Fielder B, Hopkins IJ (1993) Landau-Kleffner syndrome: six patients
including discordant monozygotic twins. Pediatric Neurology 9:49-53.
- Landau WM, Kleffner FR (1957) Syndrome of acquired aphasia with convulsive disorder in
children. Neurology 7:523-30.
- Bourgeois BF, Landau WM (2004) Landau-Kleffner syndrome and temporal cortical volume
reduction: cause or effect? Neurology. 2004 Oct 12;63(7):1152-3.
- Takeoka M, Riviello JJ Jr, Duffy FH, Kim F, Kennedy DN, Makris N, Caviness VS Jr, Holmes
GL.Bilateral volume reduction of the superior temporal areas in Landau-Kleffner syndrome.
Neurology. 2004 Oct 12;63(7):1289-92.
- Hulse WC, Heller T.Dementia infantilis. J Nerv Ment Dis. 1954 Jun;119(6):471-7.
- DeSanctis S (1908) Dementia pracocissima catatonica oder Katatonie des frueheren
Kindesalters? Folia Neuro-Biologica, (Leipzig) 2:9-12.
- Ban TA.Neuropsychopharmacology and the genetics of schizophrenia: a history of the
diagnosis of schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2004 Aug;28(5):
753-62.
- Rogers SJ (2004) Developmental regression in autism spectrum disorders. Ment Retard
Dev Disabil Res Rev. 2004;10(2):139-43.
- Mouridsen SE. Childhood disintegrative disorder.Brain Dev. 2003 Jun;25(4):225-8.
- Stefanatos GA, Kinsbourne M, Wasserstein J (2002) Acquired epileptiform aphasia: a
dimensional view of Landau-Kleffner syndrome and the relation to regressive autistic
spectrum disorders. Child Neuropsychol. 2002 Sep;8(3):195-228.
- Hendry CN (2000) Childhood disintegrative disorder: should it be considered a distinct
diagnosis? Clin Psychol Rev. 2000 Jan;20(1):77-90.
- Burd L, Fisher W, Kerbeshian J (1989)Pervasive disintegrative disorder: are Rett syndrome
and Heller dementia infantilis subtypes? Dev Med Child Neurol. 1989 Oct;31(5):609-16.
- Rapin I (1965) Dementia infantilis (Heller’s disease). In Carter CH, ed, Medical Aspects of
Mental Retardation. Charles C Thomas, Springfield IL, chapter 23, pp760-767.
- Darby JK, Clark L (1992) Autism syndrome as a final common pathway of behavioral
expression for many organic disorders. American Journal of Psychiatry 149:146-147.
- Wing, L., Yeates, S., Brierley, L.M., & Gold, J. (1976). The prevalence of early childhood
autism: comparison of administrative and epidemiological studies. Psychological Medicine,
6, 89-100.
- Bodier C, Lenoir P, Malvy J, Barthélemy C, Wiss M, Sauvage D. (2001) Autisme et
pathologies associées. Étude clinique de 295 cas de troubles envahissants du
developpment. Presse Médicale 30(24 Pt 1):1199-203.
- Simon N, Volicer L (1976) Neonatal asphyxia in the rat: greater vulnerability of males and
persistent effects on brain monoamine synthesis. Journal of Neurochemistry 26:893-900.
- Philippart M (1993) Rett syndrome associated with tuberous sclerosis in a male and in a
female: evidence for arrested motor development. American Journal of Medical Genetics 48:
229-230.
- Risch N, Spiker D, Lotspeich L, Nouri N, Hinds D, Hallmayer J, Kalaydjieva L, McCague P,
Dimiceli S, Pitts T, Nguyen L, Yang J, Harper C, Thorpe D, Vermeer S, Young H, Hebert J, Lin
A, Ferguson J, Chiotti C, Wiese-Slater S, Rogers T, Salmon B, Nicholas P, Myers RM, et al.
(1999) A genomic screen of autism: evidence for a multilocus etiology. American Journal of
Human Genetics. 65:493-507.
- Stoltenberg SF, Burmeister M. (2000) Recent progress in psychiatric genetics-some hope
but no hype. Hum Mol Genet 2000 Apr 12;9(6):927-35
- Buxbaum JD, Silverman JM, Smith CJ, Kilifarski M, Reichert J, Hollander E, Lawlor BA,
Fitzgerald M, Greenberg DA, Davis KL. (2001) Evidence for a susceptibility gene for autism on
chromosome 2 and for genetic heterogeneity. American Journal of Human Genetics 68:1514-
1520 (Erratum in: Am J Hum Genet 2001 Aug;69(2):470).
- Philippe A, Guilloud-Bataille M, Martinez M, Gillberg C, Rastam M, Sponheim E, Coleman M,
Zappella M, Aschauer H, Penet C, Feingold J, Brice A, Leboyer (2002) Analysis of ten
candidate genes in autism by association and linkage. American Journal of Medical
Genetics 114:125-128
- Fisher SE.Tangled webs: tracing the connections between genes and cognition. Cognition.
2006 Sep;101(2):270-97.
3 - Genetics
The belief is strong that autism is a genetic disorder.
But Autism is not 100 percent concordant in identical
twins, which means it is not the result of a single
defective gene [1]. The finding of even one pair of
identical twins who are discordant for any disorder
provides the counterexample that disproves a single
gene etiology. Greenberg et al (2001) noted a higher
concordance of autism in fraternal twins than would be
expected in the general population, which should
indicate that environmental influences are more
significant than genetic factors [2]. If environmental
factors were not involved, the concordance rate for
fraternal twins should not be greater than between
single-born siblings in families in which autism has
occurred more than once.
Norman (1982) noted that perinatal hazards are
increased for twins and suggested that therefore twins
are an imperfect model for genetic versus
environmental studies of things like intelligence [3].
That concordance is higher in identical than fraternal
twins reflects factors such as the limited capacity of a
shared placenta to withstand environmental hazards
like anoxia or prenatal infections. Davis et al. (1995)
found that twins who both develop schizophrenia were
more likely to have shared a single placenta and
chorionic sack in utero [4]. Autism becomes evident
years earlier than schizophrenic disorders and is
therefore even more likely related to prenatal
environment. Of the identical twins studied by
Belmonte and Carper (2006), the more seriously
affected twin was not breathing at birth [1]. Further,
he failed a hearing test at 9 months of age, which was
the impetus for the parents seeking advice, and
suggests that auditory system impairment might be
related to not breathing at birth.
Autism has been noted as a complication of the
genetic disorder phenylketonuria [5-9]. Gillberg and
Coleman (1996) compiled a table of other medical
disorders associated with autism, many of which are
assumed due to inborn errors of metabolism [10]. But
at least some of these medical conditions may be
mistakenly thought of as genetic. For example
Migeon et al. (1995) and Subramaniam et al. (1997)
described a pair of identical twin girls in which one had
Rett syndrome but the other was developing normally
still at the age of six [11, 12]. Also Feekery et al.
(1993) reported Landau-Kleffner syndrome in one but
not the other of identical twins [13].
Landau and Kleffner (1957) described loss of normal
language acquisition with seizure disorder developing
between 2 and 7 years of age, and arrested
development of the temporal lobes [14-16].
Landau-Kleffner syndrome (LKS) may or may not
include autistic behaviors [15].
Dementia infantilis, described by Heller (1908) and
DeSanctis (1908), was an earlier designation for what
is now referred to as disintegrative disorder [17-18].
Dementia infantilis is a term based on Kraepelin's
"dementia praecox," later, and euphemistically,
renamed schizophrenia [19]. Heller and DeSanctis
described autism in children 35 years before Kanner's
report, but in terms of the earliest manifestation of
schizophrenia.
Landau-Kleffner syndrome (LKS) and Heller
Syndrome are designations that predate use of the
term disintegrative disorder, but refer to children who
developed normally at first but then regressed with
loss of acquired language with or without autistic
behaviors [20-24]. Rapin (1965) compiled a table of
diverse conditions found associated with Heller
syndrome and proposed that this condition is the
result of a variety of diseases that affect the central
nervous system [25]. Thus as Darby and Clark
(1992) pointed out, whether present from birth or
appearing after a normal period of development,
autistic disorder appears to be the final common
expression of many conditions that all result in
impairment of brain systems involved in social
interactions and language [26].
Male gender is a genetic predisposition for autism.
Epidemiologic surveys from that of Wing et al (1976)
to Bodier et al (2001) reveal that autism is more
common in males than females [27, 28]. But males
are more vulnerable to a number of developmental
disorders. According to the DSM-IV Diagnostic and
Statistical Manual of Mental Disorders (American
Psychiatric Association 1994), most psychiatric
disorders occur more frequently in males than females.
In my own research (Simon & Volicer 1976) we found
male laboratory rats more vulnerable to neonatal
asphyxia than females; this was dramatically evident in
early growth retardation of males [29]. After
maturation we found increased serotonin synthesis in
the brain only in male rats subjected to neonatal
asphyxia. No visible damage could be seen in the
brain, although an increase in brain norepinephrine
synthesis was found after maturation in both males
and females.
Rett syndrome which affects only females, and in
which autistic behaviors are prominent, stands in
contrast to the usual preponderance of autism in
males. It has been suggested however that Rett
syndrome in males might lead to death before a
diagnosis could be made. Philippart (1993) reported
Rett syndrome associated with tuberous sclerosis in a
male and in a female [30]. Tuberous sclerosis has
long been associated with autism and may also be
more lethal in males.
Genes associated with autism are numerous, and
autism appears to result from interaction of multiple
genetic features [31-35]. Genes for large infant
heads and small maternal pelvis may be among these,
or genes for a constitution strong enough to survive
prenatal infection or trauma and anoxia at birth.
Belonging to the human race is a genetic
predisposition for autism. Perhaps an animal model of
autism could be found among gorillas or other higher
primates in which shared attention is important for
development. But the brain areas vulnerable to
environmental as well as genetic factors that impair
the capacity for social awareness and language
should be the primary focus of research on the
causes of autism.
Genes are not directly responsible for behavior.
Therefore, even in known genetic disorders
associated with autism the effect is on the brain.
What is important is to determine how the brain is
affected by all of the different metabolic disorders that
predispose a child to develop autism.
- Belmonte MK, Carper RA
(2006) Monozygotic twins with
Asperger syndrome:
differences in behaviour
reflect variations in brain
structure and function.
- Greenberg DA et al. (2001)
Excess of Twins among
Affected Sibling Pairs with
Autism: Implications for the
Etiology of Autism.
- Norman MG (1982)
Mechanisms of brain damage
in twins.
- Davis JO et al. (1995)
Prenatal development of
monozygotic twins and
concordance for
schizophrenia.
- Lowe TL et al. (1980).
Detection of phenylketonuria
in autistic and psychotic
children.
- Williams RS et al. (1980)
Autism and mental
retardation: Neuropathologic
studies performed in four
retarded persons with autistic
behavior.
- Chen CH, Hsiao KJ (1989) A
Chinese classic
phenylketonuria manifested
as autism.
- Miladi N et al. (1992)
Phenylketonuria: an
underlying etiology of autistic
syndrome. A case report.
- Leuzzi V et al. (1995)
Biochemical, clinical and
neuroradiological (MRI)
correlations in late-detected
PKU patients.
- Gillberg C, Coleman M
(1996). Autism and medical
disorders: a review of the
literature.
- Migeon BR et al. (1995)
Studies of X inactivation and
isodisomy in twins provide
further evidence that the X
chromosome is not involved
in Rett syndrome.
- Subramaniam B et al. (1997)
Neuroanatomy in Rett
syndrome: cerebral cortex
and posterior fossa.
- Feekery C et al. (1993)
Landau-Kleffner syndrome:
six patients including
discordant monozygotic twins.
- Landau WM, Kleffner FR
(1957) Syndrome of acquired
aphasia with convulsive
disorder in children.
- Bourgeois BF, Landau WM
(2004) Landau-Kleffner
syndrome and temporal
cortical volume reduction:
cause or effect?
- Takeoka M et al. (2004)
Bilateral volume reduction of
the superior temporal areas
in Landau-Kleffner syndrome.
- Hulse WC, Heller T.Dementia
infantilis.
- DeSanctis S (1908) Dementia
pracocissima catatonica oder
Katatonie des frueheren
Kindesalters?
- Ban TA (2004)
Neuropsychopharmacology
and the genetics of
schizophrenia: a history of the
diagnosis of schizophrenia.
- Rogers SJ (2004)
Developmental regression in
autism spectrum disorders.
- Mouridsen SE (2003)
Childhood disintegrative
disorder.
- Stefanatos GA et al. (2002)
Acquired epileptiform
aphasia: a dimensional view
of Landau-Kleffner syndrome
and the relation to regressive
autistic spectrum disorders.
- Hendry CN (2000) Childhood
disintegrative disorder:
should it be considered a
distinct diagnosis?
- Burd L et al. (1989) Pervasive
disintegrative disorder: are
Rett syndrome and Heller
dementia infantilis subtypes?
- Rapin I (1965) Dementia
infantilis (Heller’s disease).
- Darby JK, Clark L (1992)
Autism syndrome as a final
common pathway of
behavioral expression for
many organic disorders.
- Wing, L. et al. (1976). The
prevalence of early childhood
autism: comparison of
administrative and
epidemiological studies.
- Bodier C et al. (2001) Autisme
et pathologies associées.
Étude clinique de 295 cas de
troubles envahissants du
developpment.
- Simon N, Volicer L (1976)
Neonatal asphyxia in the rat:
greater vulnerability of males
and persistent effects on
brain monoamine synthesis.
Journal of Neurochemistry 26:
893-900.
- Philippart M (1993) Rett
syndrome associated with
tuberous sclerosis in a male
and in a female: evidence for
arrested motor development.
American Journal of Medical
Genetics 48:229-230.
- Risch N et al. (1999) A
genomic screen of autism:
evidence for a multilocus
etiology.
- Stoltenberg SF, Burmeister M.
(2000) Recent progress in
psychiatric genetics-some
hope but no hype.
- Buxbaum JD et al. (2001)
Evidence for a susceptibility
gene for autism on
chromosome 2 and for
genetic heterogeneity.
- Philippe A et al. (2002)
Analysis of ten candidate
genes in autism by
association and linkage.
- Fisher SE (2006) Tangled
webs: tracing the connections
between genes and cognition.
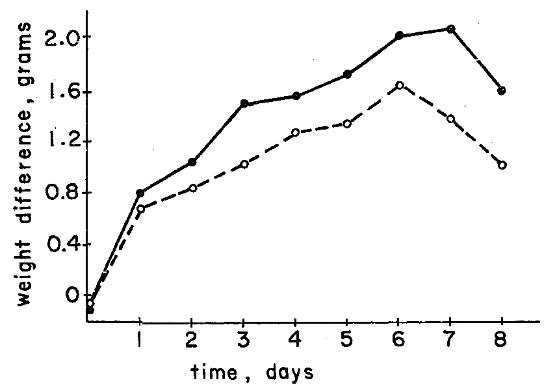
Weight differences between control and asphyxiated male and female pairs
during the first week after neonatal suffocation.
From: Simon N, Volicer L (1976) Neonatal asphyxia in the rat: greater vulnerability of males and
persistent effects on brain monoamine synthesis. Journal of Neurochemistry 26:893-900.
|
Growth retardation
of rat pups following asphyxia at
birth was more severe in males,
shown by differences in weight
from normal pups.
males
females
males
females