1 - Autism, a neurologic disorder?
Autism has not been viewed as a neurological
disorder because its definition does not include
impairment of motor movements. In fact, however,
transient delay in motor development is frequent in
children with autism, though considered "mild," and
parents concerns are often dismissed with comments
like, "Boys tend to develop slower than girls." Most
parents are aware that not all boys lag behind girls in
achieving motor milestones. However, persistent
neurological "soft signs" are common in children with
autism, indicating at least minor permanent
involvement of motor systems of the brain. Social
obliviousness and lack of communicative language
are what distinguish a child with autism from other
children with delayed motor development, and also
can be linked to neurological impairment.
Lack of fine-motor coordination is among the most
prominent of the soft neurological signs seen in
children with autism. For example, Beversdorf et al
(2001) described the large, laboriously produced
handwriting of higher functioning adults with autism
[1]. Poor motor tone (hypotonia) is characteristic of
some children with autism, who may be referred to as
"dough boys." Finger movements, often to the side of
the eyes and often referred to as part of "stimming
behaviors," may not be totally voluntary; this highly
visible characteristic often occurs as part of a
response to sudden excitement, and most likely has a
neurological basis.
Faro and Windle (1969) observed that impairment of
manual dexterity was the most prominent residual
problem in monkeys subjected to asphyxia at birth
[2]. Furthermore, the monkeys maintained for several
months or years were eventually sacrificed, and it was
found that their brains had not developed normally.
Abnormalities initially confined to the brainstem, were
referred to as "minimal." The monkeys asphyxiated at
birth appeared to "catch up," but after several months
or years, wider areas of the brain were found to be
more sparsely populated with neurons and
synapses. Many of the affected areas were the same
as those reported with abnormalities in people with
autism [3].
Myers (1972) confirmed the findings of Ranck and
Windle (1959) that a brief period of total oxygen
deprivation damages the inferior colliculi and a rank-
order of other brainstem nuclei [4, 5]. Myers however
stated that involvement of brainstem nuclei was not
characteristic of brain damage caused by anoxia
during gestation or birth; his purpose had been to
find causes and preventions of damage to the motor
systems of the cerebral cortex associated with
cerebral palsy, and he discovered that partial
interference with oxygen delivery late in gestation
produced cerebral palsy in monkeys.
Partial oxygen insufficiency has a different effect on
the brain than total oxygen deprivation; this was also
observed by Miller and Myers (1970, 1972) in adult
monkeys [6, 7]. As in the case of newborn monkeys,
brainstem damage was found with total obstruction of
oxygen delivery to the brain; however, circulation to
the heart had to be maintained to achieve this in adult
monkeys. Why the effects of insufficiency versus
total deprivation of oxygen are so radically different
doesn't at first seem to make much sense. Confusion
over the occasional finding of damage confined to the
brainstem has been discussed in the medical
literature for some time. Janzer and Friede (1980)
noted that damage is not just a matter of degree of
oxygen deficit, and they proposed "cardiac arrest
encephalopathy" as a descriptive as well as
etiological term [8].
Although Myers stated that brainstem injury was not
characteristic of anoxic birth in human children, there
are several reports of neuropathology found in
children who died in the perinatal period with
prominent damage of the inferior colliculi [9-16].
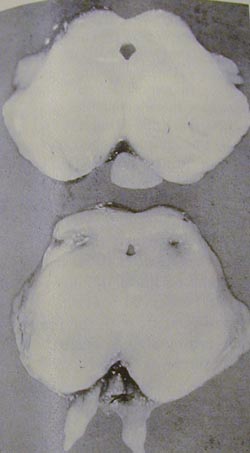
Figure 5 from the paper by Leech and Alvord (1977)
shows damage of the inferior colliculi in an infant who
died from suffocation [14] - with huge ugly holes in
the brain. It is the infant heart (not the brain) that
better withstands circulatory arrest; Miller and Myers
(1970, 1972) had to use a special technique to
protect the heart of adult monkeys in experiments that
produced total oxygen deprivation to the brain [6, 7].
A newborn can recover from a low 5-minute Apgar
score, because the infant heart is less vulnerable to
permanent damage from oxygen deprivation. The
infant brain does not recover from the effects of
asphyxia at birth [2]. The idea that "plasticity" of the
brain can make up for "minimal" or "mild" perinatal
damage is a euphemistic myth – otherwise cerebral
palsy would not be such a disaster Minimal and mild
are inappropriate adjectives for describing brain
damage of any degree.
- Beversdorf DQ et al (2001)
Brief report: macrographia in
high-functioning adults with
autism spectrum disorder.
- Faro MD and Windle WF
(1969) Transneuronal
degeneration in brains of
monkeys asphyxiated at birth.
- Kemper TL & Bauman M
(1998). Neuropathology of
infantile autism.
- Myers RE (1972) Two
patterns of perinatal brain
damage and their conditions
of occurrence.
- Ranck JB & Windle WF
(1959) Brain damage in the
monkey, Macaca mulatta, by
asphyxia neonatorum.
- Miller JR & Myers RE (1970)
Neurological effects of
systemic circulatory arrest in
the monkey.
- Miller JR & Myers RE (1972)
Neuropathology of systemic
circulatory arrest in adult
monkeys.
- Janzer RC & Friede RL
(1980) Hypotensive brain
stem necrosis or cardiac
arrest encephalopathy?
- Norman MG (1972) Antenatal
neuronal loss and gliosis of
the reticular formation,
thalamus, and
hypothalamus. A report of
three cases.
- Griffiths AD & Laurence KM
(1974) The effect of hypoxia
and hypoglycemia on the
brain of the newborn human
infant.
- Grunnet ML et al (1974) Brain
changes in newborns from
an intensive care unit.
- Schneider H et al (1975)
Anoxic encephalopathy with
predominant involvement of
basal ganglia, brain stem,
and spinal cord in the
perinatal period.
- Smith JF & Rodeck C (1975)
Multiple cystic and focal
encephalomalacia in infancy
and childhood with brain
stem damage.
- Leech RW & Alvord EC (1977)
Anoxic-ischemic
encephalopathy in the human
neonatal period, the
significance of brain stem
involvement.
- Roland EH et al (1988)
Selective brainstem injury in
an asphyxiated newborn.
- Natsume J et al (1995)
Clinical, neurophysiologic,
and neuropathological
features of an infant with
brain damage of total
asphyxia type (Myers).

From Leech & Alvord (1977) with
permission from the American
Medical Association.
|
Damage of the inferior colliculi in a
human infant (bottom) who died of
suffocation.
Damage of the inferior colliculi in a
human infant (bottom) who died of
suffocation.
From Leech & Alvord (1977) with
permission from the American
Medical Association.
>>
- Beversdorf DQ, Anderson JM, Manning SE, Anderson SL, Nordgren RE, Felopulos GJ,
Bauman ML. Brief report: macrographia in high-functioning adults with autism spectrum
disorder. J Autism Dev Disord. 2001 Feb;31(1):97-101.
- Faro MD & Windle WF (1969) Transneuronal degeneration in brains of monkeys
asphyxiated at birth. Experimental Neurology 24:38-53.
- Kemper TL, Bauman M (1998). Neuropathology of infantile autism. Journal of
Neuropathology and Experimental Neurology 57:645-652 .
- Myers RE (1972) Two patterns of perinatal brain damage and their conditions of
occurrence. American Journal of Obstetrics and Gynecology 112:246-276.
- Ranck JB, Windle WF (1959). Brain damage in the monkey, Macaca mulatta, by asphyxia
neonatorum. Experimental Neurology 1:130-154.
- Miller JR, Myers RE (1970) Neurological effects of systemic circulatory arrest in the
monkey. Neurology 20:715-724.
- Miller JR, Myers RE (1972) Neuropathology of systemic circulatory arrest in adult
monkeys. Neurology 22:888-904.
- Janzer RC, Friede RL. Hypotensive brain stem necrosis or cardiac arrest
encephalopathy? Acta Neuropathol (Berl). 1980;50(1):53-6.
- Norman MG (1972) Antenatal neuronal loss and gliosis of the reticular formation,
thalamus, and hypothalamus. A report of three cases. Neurology (Minneapolis) 22:910-
916.
- Griffiths AD, Laurence KM (1974) The effect of hypoxia and hypoglycemia on the brain of
the newborn human infant. Developmental Medicine and Child Neurology 16:308-319.
- Grunnet ML, Curless RG, Bray PF, Jung AL (1974) Brain changes in newborns from an
intensive care unit. Developmental Medicine and Child Neurology 16:320-328.
- .Schneider H, Ballowitz L, Schachinger H, Hanefield F, Droeszus J-U (1975) Anoxic
fcencephalopathy with predominant involvement of basal ganglia, brain stem, and spinal
cord in the perinatal period. Acta Neuropathologica (Berlin) 32:287-298.
- Smith JF, Rodeck C (1975) Multiple cystic and focal encephalomalacia in infancy and
childhood with brain stem damage. Journal of the neurological sciences 25:377-88
- Leech RW, Alvord EC (1977) Anoxic-ischemic encephalopathy in the human neonatal
period, the significance of brain stem involvement. Archives of Neurology 34:109-113.
- Roland EH, Hill A, Norman MG, Flodmark O, MacNab AJ (1988) Selective brainstem
injury in an asphyxiated newborn. Annals of Neurology 23:89-92.
- Natsume J, Watanabe K, Kuno K, Hayakawa F, Hashizume Y (1995) Clinical,
neurophysiologic, and neuropathological features of an infant with brain
damage of total asphyxia type (Myers). Pediatric Neurology 13:61-64.
BIg ugly holes in the
midbrain auditory pathway
Ugly holes in the brain
>>