- Windle WF (1969a) Brain damage by asphyxia at birth. Scientific American 221(#4):76-
84.
- Myers RE (1972) Two patterns of perinatal brain damage and their conditions of
occurrence. American Journal of Obstetrics and Gynecology 112:246-276
- Mirsky AF, Orren MM, Stanton L, Fullerton BC, Harris S, Myers RE (1979) Auditory evoked
potentials and auditory behavior following prenatal and perinatal asphyxia in rhesus
monkeys. Developmental Psychobiology 12:369-379.
- Clark SL, Hankins GD. (2003) Temporal and demographic trends in cerebral palsy--
fact and fiction. Am J Obstet Gynecol. 2003 Mar;188(3):628-33.
- Towbin A (1970) Neonatal damage of the central nervous system. In Tedeschi CG (ed)
Neuropathology: Methods and Diagnosis. Boston, Little, Brown & Co., pp 609-653.
- Kety SS (1962) Regional neurochemistry and its application to brain function. In French,
JD, ed, Frontiers in Brain Research. New York: Columbia University Press, pp 97-120.
- Sokoloff L (1981) Localization of functional activity in the central nervous system by
measurement of glucose utilization with radioactive deoxyglucose. Journal of Cerebral
Blood Flow and Metabolism 1:7-36.
- Pan CL, Kuo MF, Hsieh ST. Auditory agnosia caused by a tectal germinoma. Neurology.
2004 Dec 28;63(12):2387-9.
- Meyer B, Kral T, Zentner J. (1996) Pure word deafness after resection of a tectal plate
glioma with preservation of wave V of brain stem auditory evoked potentials. Journal of
Neurology, Neurosurgery and Psychiatry. 61:423-4.
- Johkura K, Matsumoto S, Hasegawa O, Kuroiwa Y. (1998) Defective auditory recognition
after small hemorrhage in the inferior colliculi. Journal of the Neurological Sciences.
161:91-6
- Masuda S, Takeuchi K, Tsuruoka H, Ukai K, Sakakura Y. (2000) Word deafness after
resection of a pineal body tumor in the presence of normal wave latencies of the
auditory brain stem response. The Annals of otology, rhinology, and laryngology. 2000
Dec;109(12 Pt 1):1107-12
- Vitte E, Tankéré F, Bernat I, Zouaoui A, Lamas G, Soudant J. Midbrain deafness with
normal brainstem auditory evoked potentials. Neurology 2002;58:970–973.
- Hoistad DL, Hain TC (2003) Central hearing loss with a bilateral inferior colliculus
lesion. Audiol Neurootol 2003 Mar-Apr; 8(2):111-223
- Kimiskidis VK, Lalaki P, Papagiannopoulos S, Tsitouridis I, Tolika T, Serasli E, Kazis D,
Tsara V, Tsalighopoulos MG, Kazis A. Sensorineural hearing loss and word deafness
caused by a mesencephalic lesion: clinicoelectrophysiologic correlations. Otol
Neurotol. 2004 Mar;25(2):178-82.
- Musiek FE et al (2004) Central deafness associated with a midbrain lesion. J Am Acad
Audiol 2004 feb; 15(2):133-151.
- Howe JR, Miller CA. Midbrain deafness following head injury. Neurology. 1975 Mar;25(3):
286-9.
- Ranck JB, Windle WF (1959). Brain damage in the monkey, Macaca mulatta, by
asphyxia neonatorum. Experimental Neurology 1:130-154.
- Jacobson HN & Windle WF (1960) Responses of foetal and new-born monkeys to
asphyxia. The Journal of Physiology (London) 153:447-456.
1 - Puzzling results of research on asphyxia at
birth
Windle (1969) and Myers (1972) found that a brief
period of total asphyxia at birth selectively damages
the inferior colliculus in monkeys [1, 2]. Figure xx in
chapter 8 is from the article by Windle and shows the
damage caused by asphyxia compared to the
appearance of the inferior colliculus in a normal
monkey. Damage to the inferior colliculus has also
been observed in human infants who died at birth.
Figure xx shows damage in the inferior colliculi of a
human infant who died of suffocation. Thus damage
to the inferior colliculi caused by asphyxia at birth in
monkeys also happens in humans. Mirsky et al.
(1979) demonstrated auditory evoked potential
abnormalities in monkeys asphyxiated at birth
comparable to those in children with autism [3]; the
monkeys had known damage in the inferior colliculi.
The issue of obstetrical complications can provoke
extreme controversy when proposed as an etiologic
factor in autism or any other developmental disorder
[4]. Injury at birth is a taboo subject. However,
accidents such as breech birth, malpresentation of
the head in the birth canal, premature separation of
the placenta, or prolapse of the umbilical cord make
birth one of the most hazardous experiences of life;
many of these situations were discussed by Towbin
(1970) in Tedeschi’s textbook of neuropathology [5].
Figure xx in chapter 8 illustrates the kind of injury to
the head that can occur during a traumatic birth.
Windle (1969) pointed out that the human maternal
pelvis only marginally accommodates the large size of
the infant head, and even when it may have appeared
there were no major complications at birth, a brief
period of oxygen deprivation can have taken place; if
so, the inferior colliculi may be the only structure
affected in the brain [1]. Myers (1972) referred to
damage restricted to the inferior colliculus and other
brainstem nuclei as minor [2].
But visible damage anywhere in the brain cannot be
regarded as minor when disorders as serious as
autism are attributed to neurochemical defects in the
absence of clearcut lesions. Asphyxia insufficient to
produce visible lesions of the inferior colliculi may still
cause decrements in function. Furthermore, high
blood flow and metabolic rate in the inferior colliculi
indicates that this small area has important functions
for the brain as a whole [6, 7].
Monkeys are not expected to understand speech, or
learn to talk, and damage to the auditory system may
not be as debilitating for subhuman primates as for a
human infant. But the effects of visible damage in the
inferior colliculi merit investigation as much as any
lesion of a higher cortical brain area. As discussed in
chapter xx above (section xx), at least ten cases have
been reported of adults who lost the capacity for
speech understanding after damage to the inferior
colliculi [8-16].. Damage caused by asphyxia at birth
and involving only the inferior colliculi therefore
cannot be considered minor, especially in an infant
with no previous experience with spoken language.
In their investigations of asphyxia at birth Windle and
co-workers (Ranck & Windle 1959, Jacobson &
Windle 1960) intended to produce an animal model of
spastic cerebral palsy, with the objective of then
looking for ways to prevent this tragedy in human
children [17 18]. Their hypothesis was that oxygen
deprivation around the time of birth would damage the
motor areas of the cerebral cortex. Cerebral palsy is
known to result from damage to the motor areas of
the cerebral cortex, but reproducing this pattern of
brain damage was elusive.
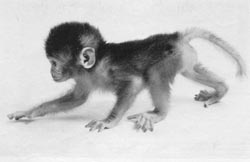
Monkeys subjected to several minutes of total
asphyxia displayed a transient form of hypotonic
cerebral palsy. Figure xx from the article by Windle
(1969) shows an infant monkey with hypotonic
muscles unable to get up on all four limbs. Monkeys
subjected to such episodes of asphyxia slowly gained
control of motor functions for normal locomotion, but
residual deficits in memory remained. Asphyxia did
not cause spastic cerebral palsy as anticipated, and
damage within the brain was not evident until careful
examination of the brainstem revealed the lesions in
the inferior colliculi with lesser involvement of other
brainstem nuclei. Parents of human children with
delay in early motor development are rightfully
concerned, even when pediatricians insist there is no
cause for worry.
Myers (1972), a member of Windle's team, began a
new series of experiments with fetal monkeys. He
used a technique to partially block blood flow to the
fetus, thus simulating placental insufficiency. These
monkeys were born with true spastic cerebral palsy,
and the expected brain damage was found in the
cerebral cortex [2]. In Myers' experiments partial
disruption of circulation with insufficient delivery of
oxygen was inflicted, and persisted over a longer
period of time.
Figure xx is from the paper by Myers and shows
damage of the inferior colliculi caused by 12 minutes
of total asphyxia at birth. Myers confirmed once again
the finding of brainstem pathology but rejected any
possible importance of damage to the inferior colliculi
or other brainstem nuclei, because he believed
episodes of brief total asphyxia never occurred in real
life. Myers referred to the selective damage of
brainstem nuclei as lesions affecting a monotonous
rank order of subcortical sites, and stated that this
bore no resemblance to damage of the cerebral
cortex seen in human cases.
As stated above in chapter xx (section xx), there are
several reports of damage confined to the brainstem
in infants who died in early infancy; these cases are
described in chapter xx. Myers overlooked the
possibility that a brief period (or successive periods)
of total asphyxia can also occur prenatally or during a
difficult birth.
Prolonged perinatal distress is no doubt more
common and in many cases may precede a brief
episode of total circulatory arrest and asphyxia. Most
children with autism also show signs of minor motor
impairment; children with Asperger syndrome have
clear-cut motor impairments. Children with Asperger
syndrome have a greater involvement of motor
systems with lesser deficits in language development
and social interactions.
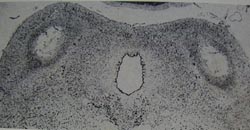
Damage found in the inferior colliculi
in monkeys subjected to sudden,
catastrophic asphyxia - inflicted by
delivering the head of infant monkeys
into a saline-filled sac, and clamping
the umbilical cord. Compare with the
appearance of the inferior colliculi in
a monkey born normally.
These pictures were published in the
October 1969 issue of the Scientific
American as part of an article by
William Windle on asphyxia at birth.
They were first published in the
article by Ranck & Windle (1959).
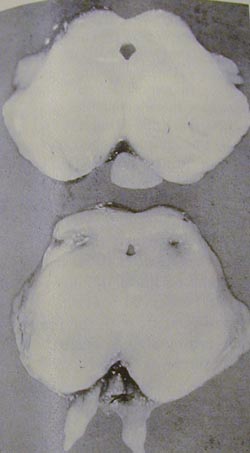
|
Damage of the inferior colliculi in a
human infant (bottom) who died of
suffocation. -->
From Leech & Alvord (1977) with
permission from the American
Medical Association.
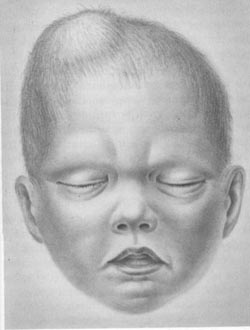
|
Cephalhematoma
From Towbin (1970)
|


- Windle WF (1969) Brain
damage by asphyxia at birth.
- Myers RE (1972) Two
patterns of perinatal brain
damage and their conditions
of occurrence.
- Mirsky AF et al. (1979)
Auditory evoked potentials
and auditory behavior
following prenatal and
perinatal asphyxia in rhesus
monkeys.
- Clark SL, Hankins GD.
(2003) Temporal and
demographic trends in
cerebral palsy--fact and
fiction.
- Towbin A (1970) Neonatal
damage of the central
nervous system.
- Kety SS (1962) Regional
neurochemistry and its
application to brain function.
- Sokoloff L (1981)
Localization of functional
activity in the central nervous
system by measurement of
glucose utilization with
radioactive deoxyglucose.
- Pan CL et al (2004) Auditory
agnosia caused by a tectal
germinoma.
- Meyer B et al (1996) Pure
word deafness after
resection of a tectal plate
glioma with preservation of
wave V of brain stem auditory
evoked potentials.
- Johkura K et al (1998)
Defective auditory recognition
after small hemorrhage in
the inferior colliculi.
- Masuda S et al (2000) Word
deafness after resection of a
pineal body tumor in the
presence of normal wave
latencies of the auditory brain
stem response.
- Vitte E et al (2002) Midbrain
deafness with normal
brainstem auditory evoked
potentials. (two case reports).
- Hoistad DL et al (2003)
Central hearing loss with a
bilateral inferior colliculus
lesion.
- Kimiskidis VK et al (2004)
Sensorineural hearing loss
and word deafness caused
by a mesencephalic lesion:
clinicoelectrophysiologic
correlations.
- Musiek FE et al (2004)
Central deafness associated
with a midbrain lesion.
- Howe JR, MillerCA (1975)
Midbrain deafness following
head injury.
- Ranck JB, Windle WF (1959).
Brain damage in the monkey,
Macaca mulatta, by asphyxia
neonatorum.
- Jacobson HN & Windle WF
(1960) Responses of foetal
and new-born monkeys to
asphyxia.


Normal monkey
Monkey with motor delay