3 - Wernicke's encephalopathy
Wernicke (1881a) discovered symmetric bilateral
damage of brainstem areas in a young woman who
died several months after ingesting sulfuric acid, and
he found the same bilateral pattern of damage in the
brains of two men who had been chronic users of
alcohol to the point of intoxication [1, 2]. The
brainstem centers affected were the same nuclei of
high metabolic rate later identified through use of the
autoradiographic techniques for blood flow and
deoxyglucose uptake. Note that the finding of
brainstem damage caused by intoxication was a new
discovery not directly related to Wernicke's earlier
analysis (in 1874) of cortical association tracts
involved in aphasic disorders [3].
Bilateral involvement of the brainstem nuclei of high
metabolic rate has become a well recognized pattern
of pathology known as Wernicke's encephalopathy.
Wernicke’s observations have been confirmed by
many subsequent investigators [4-9]. This brainstem
pattern is most often associated with chronic alcohol
abuse, but can also be caused by deficiency of vitamin
B1 (thiamine). Wernicke-like patterns of damage have
further increasingly been noted in cases where death
resulted from exposure to toxic substances [10-12].
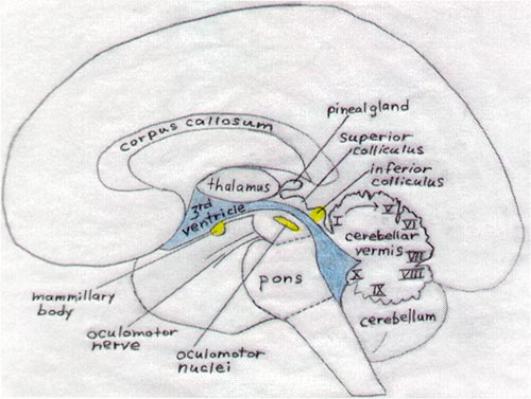
Figure 9 depicts a midline view of the brain and
brainstem structures affected in Wernicke's
encephalopathy. The mammillary bodies are usually
most prominently affected, but the oculomotor nuclei,
inferior colliculi, inferior olives, and cerebellum are
also often damaged. The pattern and degree of
involvement of these structures varies from case to
case. Variability in vulnerability can best be explained
in terms of the protective feedback mechanisms that
go into action during a chronic course of exposure to
alcohol or any other situation that impairs cerebral
metabolism.
If the high rate of metabolism in the inferior colliculus
supports some crucial function for survival (auditory
attention, orientation, awareness, or even
consciousness), evolutionary adaptations may have
led to development of mechanisms to prevent lapses
in function. Metabolic rate in the mammillary bodies is
not as high, and consolidation of short-term to long-
term memory may not be as immediately essential for
survival as auditory surveillance; thus the memory
consolidation function will suffer in favor of systems
that sense changes in the environment.
Protective mechanisms often involve vasodilation to
increase blood supply [13, 14]. The same mechanism
also leads to the swollen red "whiskey nose" of chronic
alcoholics. If the protective dilation of blood vessels
intensifies or persists, it can lead to small
hemorrhages due to bursting of some of the blood
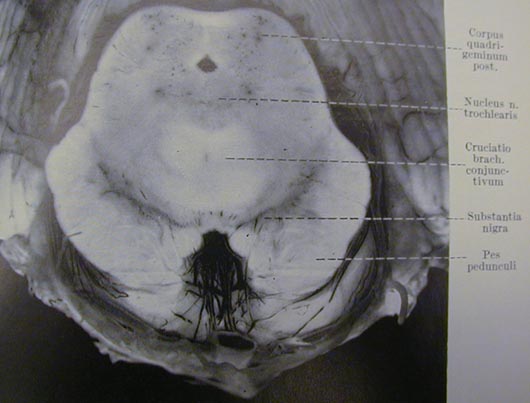
capillaries. Figure 8 (from Kant's 1933 article) is a
photograph showing the hemorrhagic damage in the
inferior colliculi and tissue surrounding the aqueduct.
Figure 10, from Vortmeyer et al,1992 [15], shows
intense damage in the inferior colliculi caused by a
catastrophic and rapid depletion of thiamine in a
terminally ill patient maintained on intravenous
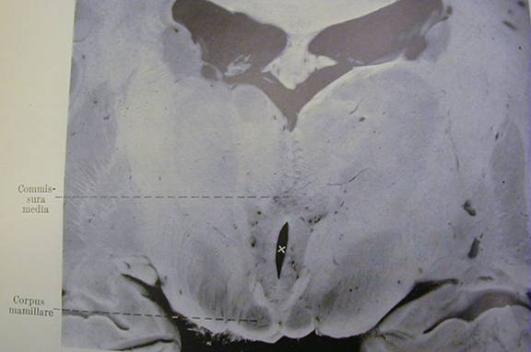
feeding. Figure 16 (from Kant 1933) shows the more
intense damage in the mammillary bodies caused by
chronic alcohol intoxication.
Cerebellar involvement is also commonly observed as
part of Wernicke’s encephalopathy. Cavanagh et al.
(1997) discussed an array of toxic substances that
deplete Purkinje cells and damage the cerebellar
vermis; these include L-beta-methylaminoalanine
(BMAA), penitrem A produced by Penicillium
crustosum, a fungus that contaminates food,
phencyclidine (PCP), and the plant-derived indole
terpenes ibogaine and harmaline [16]. The finding of
cerebellar involvement in children with autism, and of
autistic disorder in children exposed to alcohol and
other toxic substances during gestation is another
reason to consider degradation of function within the
brainstem nuclei of high metabolic rate as part of the
brain impairment in autism.
Figure 9 - Diagram showing brainstem sites affected in Wernicke's encephalopathy
|
Figure 8 - From Kant (1933). Corpora quadrigeminae posterior, another name for
|
Figure 10 - From Vortmeyer et al. (1992)
Damage to the inferior colliculi
in a human patient maintained on
prolonged parenteral feeding
lacking vitamin B1
|
Figure 14 - From Kant (1933), showing the usual site of most severe damage in
Wernicke's encephalopathy, the mammillary bodies (corpus mamillare).
|

- Wernicke C (1881a) Die
acute, haemorrhagische
Poliencephalitis superior.
Lehrbuch der
Gehirnkrankheiten für Ärzte
und Studirende,Band II.
- Brody IA, Wilkins RH. (1968)
Wernicke's encephalopathy.
- Wernicke C (1874) The
symptom complex of
aphasia,.
- Gamper (1928) Zur Frage
der Polioencephalitis
haemorrhagica der
chronischen Alkoholiker.
Anatomische Befunde beim
alkoholischen Korsakow
und ihre Beziehungen zum
klinischen Bild.
- Kant F (1933) Die
Pseudoencephalitis
Wernicke der Alkoholiker.
(polio-encephalitis
haemorrhagica superior
acuta).
- Malamud N, Skillicorn SA
(1956). Relationship
between the Wernicke and
the Korsakoff Syndrome.
- Torvik A (1987) Topographic
distribution and severity of
brain lesions in Wernicke's
encephalopathy.
- Victor M, et al. (1989) The
Wernicke-Korsakoff
syndrome and related
neurologic disorders due to
alcoholism and
malnutrition, 2nd ed,
- Butterworth RF (1993)
Pathophysiology of
cerebellar dysfunction in the
Wernicke-Korsakoff
syndrome.
- Franken L (1959) Étude
anatomique d'un cas
d'intoxication par le bromure
de méthyle.
- Goulon M et al. (1975).
Intoxication par le bromure
de methyl: Trois
observations, dont une
mortelle. Etude neuro-
pathologique d'un cas de
stupeur avec myoclonies,
suivi pendent cinq ans.
- Squier MV et al. (1992)
Case report:
neuropathology of methyl
bromide intoxication.
- Hakim AM (1986) Effect of
thiamine deficiency and its
reversal on cerebral blood
flow in the rat. Observations
on the phenomena of
hyperperfusion, "no reflow,"
and delayed hypoperfusion.
- Chen Q et al. (1997)
Causality of parenchymal
and vascular changes in
rats with experimental
thiamine deficiency
encephalopathy.
- Vortmeyer AO et al. (1992)
Haemorrhagic thiamine
deficient encephalopathy
following prolonged
parenteral nutrition.
- .Cavanagh JB et al. (1997)
Selective damage to the
cerebellar vermis in chronic
alcoholism: a contribution
from neurotoxicology to an
old problem of selective
vulnerability.

the inferior colliculi
>>>
\/
\/
- Wernicke C (1881a) Die acute, haemorrhagische Poliencephalitis
superior. Lehrbuch der Gehirnkrankheiten für Ärzte und Studirende,Band
II. Kassel: Theodor Fischer, pp 229-242.
- Brody IA, Wilkins RH. (1968) Wernicke's encephalopathy. Archives of
Neurology. 19:228-32.
- Wernicke C (1874) Der aphasische Symptomencomplex, Breslau: Franck
und Weigert. Translation: The symptom complex of aphasia, in Cohen
RS & Wartofsky MW, eds (1969) Boston Studies in the Philosophy of
Science, vol 4, pp 34-97.
- Gamper (1928) Zur Frage der Polioencephalitis haemorrhagica der
chronischen Alkoholiker. Anatomische Befunde beim alkoholischen
Korsakow und ihre Beziehungen zum klinischen Bild. Deutsche Zeitschrift
für Nervenheilkunde 102:122-129.
- Kant F (1933) Die Pseudoencephalitis Wernicke der Alkoholiker. (polio-
encephalitis haemorrhagica superior acuta). Archiv für Psychiatrie und
Nervenkrankheiten 98:702-768.
- Malamud N, Skillicorn SA (1956). Relationship between the Wernicke
and the Korsakoff Syndrome. Archives of Neurology and Psychiatry, 76,
585-596.
- Torvik A (1987) Topographic distribution and severity of brain lesions in
Wernicke's encephalopathy. Clinical Neuropathology 6:25-29.
- Victor M, Adams RD, Collins GH (1989) The Wernicke-Korsakoff
syndrome and related neurologic disorders due to alcoholism and
malnutrition, 2nd ed, Contemporary Neurology Series v30. Philadelphia,
PA : F.A. Davis Co.
- Butterworth RF (1993) Pathophysiology of cerebellar dysfunction in the
Wernicke-Korsakoff syndrome. Canadian Journal of Neurological
Sciences 20 Suppl 3:S123-S126.
- Franken L (1959) Étude anatomique d'un cas d'intoxication par le
bromure de méthyle. Acta Neurologica et Psychiatrica Belgica 59:375-
383.
- Goulon M, Nouailhat R, Escourolle R, Zarranz-Imirizaldu JJ, Grosbuis S,
Levy-Alcover MA (1975). Intoxication par le bromure de methyl: Trois
observations, dont une mortelle. Etude neuro-pathologique d'un cas de
stupeur avec myoclonies, suivi pendent cinq ans. Revue Neurologique
(Paris) 131:445-468.
- Squier MV, Thompson J, Rajgopalan B. (1992) Case report:
neuropathology of methyl bromide intoxication. Neuropathology and
Applied Neurobiology 18: 579-584.
- Hakim AM (1986) Effect of thiamine deficiency and its reversal on
cerebral blood flow in the rat. Observations on the phenomena of
hyperperfusion, "no reflow," and delayed hypoperfusion. Journal of
Cerebral Blood Flow and Metabolism 6:79-85.
- Chen Q, Okada S, Okeda R (1997) Causality of parenchymal and
vascular changes in rats with experimental thiamine deficiency
encephalopathy. Pathology International 47:748-756
- Vortmeyer AO, Hagel C, Laas R (1992) Haemorrhagic thiamine deficient
encephalopathy following prolonged parenteral nutrition. Journal of
Neurology, Neurosurgery and Psychiatry 55:826-829.
- .Cavanagh JB, Holton JL, Nolan CC (1997) Selective damage to the
cerebellar vermis in chronic alcoholism: a contribution from
neurotoxicology to an old problem of selective vulnerability.
Neuropathology and Applied Neurobiology 23:355-363.