- Meyer B et al. (1996) Pure
word deafness after resection
of a tectal plate glioma with
preservation of wave V of
brain stem auditory evoked
potentials. - Masuda S et al. (2000) Word
deafness after resection of a
pineal body tumor in the
presence of normal wave
latencies of the auditory brain
stem response. - Johkura K, et al. (1998)
Defective auditory recognition
after small hemorrhage in the
inferior colliculi. - Pan CL et al. (2004) Auditory
agnosia caused by a tectal
germinoma. - Hu CJ et al. (1997) Traumatic
brainstem deafness with
normal brainstem auditory
evoked potentials. - Vitte E, et al.(2002) Midbrain
deafness with normal
brainstem auditory evoked
potentials. - Coslett HB et al. (1984) Pure
word deafness after bilateral
primary auditory cortex
infarcts. - Denes G, Semenza C. (1975)
Auditory modality-specific
anomia: evidence from a
case of pure word deafness. - Cocito D et al.(1990)
Hematoma of the inferior
colliculus: uncommon cause
of trochlear nerve deficit and
contralateral sensory
hemisyndrome. - Champoux F et al. (2007).
Auditory processing in a
patient with a unilateral lesion
of the inferior colliculus. - Hashimoto T et al. (1995)
Development of the
brainstem and cerebellum in
autistic patients. - Gaffney GR et al. (1988)
Morphological evidence for
brainstem involvement in
infantile autism. - Abell F et al. (1999) The
neuroanatomy of autism: a
voxel-based whole brain
analysis of structural scans. - Aylward EH et al. (1999) MRI
volumes of amygdala and
hippocampus in non-mentally
retarded autistic adolescents
and adults. - Elia M et al. (2000) Clinical
correlates of brain
morphometric features of
subjects with low-functioning
autistic disorder. - Simon EN. (2005) Auditory
agnosia caused by a tectal
germinoma.
5 - Word deafness and the inferior colliculi
At least thirteen cases have been reported, of loss of
speech understanding following bilateral damage of
the inferior colliculi, all in people with previously normal
language. The case reports are summarized in
chapter 8 above. Inability to understand spoken
language is often referred to as "word deafness."
Meyer et al. (1996) and Masuda et al. (2000) reported
loss of speech comprehension following accidental
destruction of the inferior colliculi during surgery for
removal of tumors [1, 2]. Johkura et al. (1998)
reported a case of traumatic injury to the inferior
colliculi suffered in a skiing accident [3].
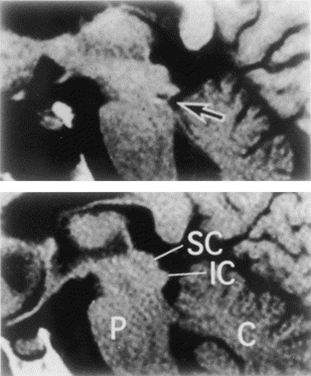
In December 2004 Pan et al. reported auditory
agnosia in a young boy who developed a cancerous
growth of the midbrain that involved both inferior
colliculi [4]. Removal of the abnormal tissue was
successful in this case, with slow but steady recovery
of auditory discrimination. Pan et al. cited the cases of
Meyer et al., Masuda et al., and Johkura et al., plus
those of Hu et al. (1997) and Vitte et al. (2002) [5, 6].
The case reported by Hu et al. was the result of
traumatic injury in a motor vehicle accident [5]. Vitte et
al. reported two cases, one the result of head injury,
the other from hemorrhage following surgery [6].
Meyer et al. commented that they were aware of three
other cases of pure word deafness with lesions
restricted to the inferior colliculi, but did not give
citations to other published reports [1]. Johkura et al.
reviewed the literature on verbal auditory agnosia, first
reported with left temporal lobe damage that
disconnected the language receptive area from
subcortical auditory input and inputs across the corpus
callosum from the right temporal lobe. Later it was
found that verbal auditory agnosia most often involved
bilateral temporal lobe damage, or disruption of the
auditory pathway from the medial geniculate bodies of
the thalamus [7, 8]. The cases of word deafness
following damage of the inferior colliculi in the 13 case
reports above, indicate that disruption even at the
midbrain level can interfere with language
comprehension.
Word deafness results only from bilateral damage of
the inferior colliculi [9, 10]. Champoux et al. (2007) did
extensive testing of a 12-year-old child with traumatic
injury of the right inferior colliculus. The child did not
display any neurological dysfunction, but speech
comprehension was impaired in the presence of
competing sounds.
Loss of function within the inferior colliculi present from
birth might be expected to prevent acquisition of
language through the normal channel of hearing.
Lesions of the inferior colliculi caused during a
traumatic birth might be visible in MRI scans, but might
also be overlooked when clear-cut damage to wider
areas of the brain are evident.
Impairment of function without visible damage within
the inferior colliculi probably would not be seen in MRI
scans. However, decreased volume of brainstem
areas in individuals with autism have been determined
by measurements of MRI scans [11-15]. This evidence
supports the usefulness of considering the perinatal
vulnerability of brainstem nuclei, and impaired function
of the inferior colliculi in the developmental language
disorder of children with autism. In their reply to my
letter on auditory agnosia resulting from a germinoma
growth into the tectum, Pan and Hsieh commented:
spoken language should be a primary focus of
research in autism. Results of existing diverse studies
of the auditory system may be useful although most
such research was not about autism.
At least thirteen cases have been reported, of loss of
speech understanding following bilateral damage of
the inferior colliculi, all in people with previously normal
language. The case reports are summarized in
chapter 8 above. Inability to understand spoken
language is often referred to as "word deafness."
Meyer et al. (1996) and Masuda et al. (2000) reported
loss of speech comprehension following accidental
destruction of the inferior colliculi during surgery for
removal of tumors [1, 2]. Johkura et al. (1998)
reported a case of traumatic injury to the inferior
colliculi suffered in a skiing accident [3].
In December 2004 Pan et al. reported auditory
agnosia in a young boy who developed a cancerous
growth of the midbrain that involved both inferior
colliculi [4]. Removal of the abnormal tissue was
successful in this case, with slow but steady recovery
of auditory discrimination. Pan et al. cited the cases of
Meyer et al., Masuda et al., and Johkura et al., plus
those of Hu et al. (1997) and Vitte et al. (2002) [5, 6].
The case reported by Hu et al. was the result of
traumatic injury in a motor vehicle accident [5]. Vitte et
al. reported two cases, one the result of head injury,
the other from hemorrhage following surgery [6].
Meyer et al. commented that they were aware of three
other cases of pure word deafness with lesions
restricted to the inferior colliculi, but did not give
citations to other published reports [1]. Johkura et al.
reviewed the literature on verbal auditory agnosia, first
reported with left temporal lobe damage that
disconnected the language receptive area from
subcortical auditory input and inputs across the corpus
callosum from the right temporal lobe. Later it was
found that verbal auditory agnosia most often involved
bilateral temporal lobe damage, or disruption of the
auditory pathway from the medial geniculate bodies of
the thalamus [7, 8]. The cases of word deafness
following damage of the inferior colliculi in the 13 case
reports above, indicate that disruption even at the
midbrain level can interfere with language
comprehension.
Word deafness results only from bilateral damage of
the inferior colliculi [9, 10]. Champoux et al. (2007) did
extensive testing of a 12-year-old child with traumatic
injury of the right inferior colliculus. The child did not
display any neurological dysfunction, but speech
comprehension was impaired in the presence of
competing sounds.
Loss of function within the inferior colliculi present from
birth might be expected to prevent acquisition of
language through the normal channel of hearing.
Lesions of the inferior colliculi caused during a
traumatic birth might be visible in MRI scans, but might
also be overlooked when clear-cut damage to wider
areas of the brain are evident.
Impairment of function without visible damage within
the inferior colliculi probably would not be seen in MRI
scans. However, decreased volume of brainstem
areas in individuals with autism have been determined
by measurements of MRI scans [11-15]. This evidence
supports the usefulness of considering the perinatal
vulnerability of brainstem nuclei, and impaired function
of the inferior colliculi in the developmental language
disorder of children with autism. In their reply to my
letter on auditory agnosia resulting from a germinoma
growth into the tectum, Pan and Hsieh commented:
- "Previous studies on structural abnormalities in
pervasive developmental disorders were
hampered by inadequate anatomical resolution of
conventional imaging tools. Functional
disturbances without obvious anatomical changes
are likely to be overlooked in some of these
conditions. With the advance of neuroimaging
techniques, particularly the magnetic resonance
imaging, these hypotheses are ready to be
tested" [16, p339].
I have posted a research proposal at http://www.
inferiorcolliculus.org/presentation.html. I have not yet
found a research group interested in undertaking such
a project.
spoken language should be a primary focus of
research in autism. Results of existing diverse studies
of the auditory system may be useful although most
such research was not about autism.
- Meyer B, Kral T, Zentner J. (1996) Pure word deafness after resection of a tectal plate glioma
with preservation of wave V of brain stem auditory evoked potentials. Journal of Neurology,
Neurosurgery and Psychiatry. 61:423-4. - Masuda S, Takeuchi K, Tsuruoka H, Ukai K, Sakakura Y. (2000) Word deafness after
resection of a pineal body tumor in the presence of normal wave latencies of the auditory
brain stem response. The Annals of otology, rhinology, and laryngology. 2000 Dec;109(12 Pt
1):1107-12. - Johkura K, Matsumoto S, Hasegawa O, Kuroiwa Y. (1998) Defective auditory recognition
after small hemorrhage in the inferior colliculi. Journal of the Neurological Sciences. 161:91-
6. - Pan CL, Kuo MF, Hsieh ST. Auditory agnosia caused by a tectal germinoma. Neurology.
2004 Dec 28;63(12):2387-9. - Hu CJ, Chan KY, Lin TJ, Hsiao SH, Chang YM, Sung SM. (1997) Traumatic brainstem
deafness with normal brainstem auditory evoked potentials. Neurology 1997;48:1448–1451. - Vitte E, Tankéré F, Bernat I, Zouaoui A, Lamas G, Soudant J. Midbrain deafness with normal
brainstem auditory evoked potentials. Neurology 2002;58:970–973. - Coslett HB, Brashear HR, Heilman KM. Pure word deafness after bilateral primary auditory
cortex infarcts. Neurology 1984;34:347–52. - Denes G, Semenza C. Auditory modality-specific anomia: evidence from a case of pure
word deafness. Cortex 1975;11:401–11. - Cocito D, Amedeo G, Gallo G, Vischia F, De Lucchi R. Hematoma of the inferior colliculus:
uncommon cause of trochlear nerve deficit and contralateral sensory hemisyndrome. Ital J
Neurol Sci. 1990 Feb;11(1):71-4. - Champoux F, Paiement P, Mercier C, Lepore F, Lassonde M, Gagne JP.Auditory processing
in a patient with a unilateral lesion of the inferior colliculus. Eur J Neurosci. 2007 Jan;25(1):
291-7. - Hashimoto T, Tayama M, Murakawa K, Yoshimoto T, Miyazaki M, Harada M, Kuroda Y (1995)
Development of the brainstem and cerebellum in autistic patients. Journal of Autism and
Developmental Disorders 25:1-18. - Gaffney GR, Kuperman S, Tsai LY, Minchin S (1988) Morphological evidence for brainstem
involvement in infantile autism. Biological Psychiatry 24:578-586. - Abell F, Krams M, Ashburner J, Passingham R, Friston K, Frackowiak R, Happe F, Frith C,
Frith U. (1999) The neuroanatomy of autism: a voxel-based whole brain analysis of
structural scans. Neuroreport. 10:1647-51 - Aylward EH, Minshew NJ, Goldstein G, Honeycutt NA, Augustine AM, Yates KO, Barta PE,
Pearlson GD. (1999) MRI volumes of amygdala and hippocampus in non-mentally retarded
autistic adolescents and adults. Neurology. 53:2145-50. - Elia M, Ferri R, Musumeci SA, Panerai S, Bottitta M, Scuderi C. Clinical correlates of brain
morphometric features of subjects with low-functioning autistic disorder. J Child Neurol.
2000 Aug;15(8):504-8. - Simon EN. Auditory agnosia caused by a tectal germinoma. Neurology. 2005 Jul 26;65(2):
339; author reply 339.